
Abstract
Background: Response rates to point-of-care clinical reminders typically decrease over time. We hypothesized that this “reminder fatigue” could be prevented by (1) applying sound human factors engineering and cognitive science principles in designing the reminder system, and (2) implementing the reminders with rigorous attention to organizational science principles.
Methods: This was a retrospective cohort enumeration from January 1, 2006, through July 31, 2012, in a set of 5 academically affiliated family medicine practices. We modeled the odds ratio of clinician action in response to a reminder according to the number of reminders issued during the encounter, the number of problems on the patient's problem list, patient age, and time (number of months since launch) using logistic regression with clustering by encounter.
Results: There were issued 988,149 reminders at 453,537 encounters during the sampling frame. Action was taken in response to 60.1% of reminders, and discussion or consideration was documented in another 26.8%. The odds ratios for action in response to reminders over time, by number of prompts during the encounter, and by number of problems were 1.01, 1.18, and 1.02, respectively. Key design features included issuing reminders only when a service was due, allowing clinicians to attend to reminders when doing so fit their workflow (vs forcing attention at a specific time), keeping reminders very short and simple (action item only, no explicative material), and a team meeting and buy-in process before each new reminder was implemented.
Conclusions: Reminder fatigue over time, with increasing numbers of reminders and with increasing complexity of patients, is not inevitable. A reminder system designed and implemented in accordance with the principles of cognitive science and human factors engineering can prevent reminder fatigue.
- Clinical Decision Support Systems
- Primary Health Care
- Quality Improvement
- Reminder Systems
- User–Computer Interface
That point-of-care reminders to clinicians can improve rates of delivery of screening and prevention services, and of services recommended by evidence-based practice guidelines, has long been established.1⇓⇓⇓⇓–6 Improvement in patient outcomes has been limited, however, because clinician and clinical care team response rates to reminders are variable and often much lower than desired.7,8 A number of barriers to successful implementation of clinical reminder systems (CRSs) have been identified.9,10 In this article we address 1 specific problem with CRS implementation: reminder fatigue, the decrease in response rates to reminders with increasing numbers of reminders and the decline in response rates over time.10,11 In addition, “alert fatigue”12 is a commonly observed phenomenon, and some authors have explicitly recommended limiting the number of reminders, integrating reminders into workflow, minimizing false alarms, conducting usability analyses, or applying formal human–computer interaction analyses to mitigate it.10
We designed and implemented a CRS intended to cover a wide range of screening, prevention, and chronic disease management interventions. Because it was intended to be used in a busy family medicine setting with patients who have multiple chronic conditions, and hence likely to have multiple reminders relevant to their care, we sought a design and implementation approach that would limit reminder fatigue to the greatest degree possible. We hypothesized that reminder fatigue could be minimized by rigorously applying basic principles of cognitive science in the design and implementation.
Methods
Setting
This project was conducted in 5 off-campus family medicine clinics affiliated with a large, midwestern academic medical center. Two sites serve suburban, largely educated populations; 1 is located in an urban underserved area; and 2 are in small towns/rural settings. The urban site and 1 rural site serve large numbers of Medicaid and uninsured patients. Two (the urban site and 1 small town) are residency education sites, but the majority of visits in all 5 sites are with attending physicians. A total of 47 attending physicians and 8 nurse practitioners or physician assistants practiced in the 5 sites during the time the data were collected. All the sites are connected to the medical center via high-speed networking and during the study period used the medical center's homegrown electronic medical record system (which at the time did not have CRS capability).
Design and Implementation
We consulted with a human factors engineer experienced in the design of information presentation systems in aviation and discussed our plans and ideas with colleagues in the University of Michigan's Decision Consortium.13 After the initial launch and approximately a year of experience with the system, we conducted a cognitive task analysis14 of how family physicians structured office visits and acquired patient-specific information before and during visits. The methods and findings are detailed elsewhere15; briefly, the Task Diagram tool was used, with specific focus on information handling during visits. The findings were used in ongoing improvement of implementation.
This combined formal and informal design process led us to understand that clinical reminders are not at all the simple intervention they might at first seem. Though often compared with checklists in aviation, reminders for preventive or chronic disease management services in primary care differ in important ways. They are often task-discordant, that is, they direct attention to matters other than those for which the patient presents. Task flow in clinical practice is context-dependent and highly nonlinear; decisions must be made with limited or unreliable evidence under changing circumstances,16 and addressing a reminder may require interaction with a team member who is not present when the reminder is presented—in contrast to the deliberately highly routinized processes of airliner piloting. Aviation processes are deliberately designed to reduce cognitive workload; that certainly cannot be said of primary care. In the primary care setting clinical reminders are powerful stimuli being introduced into an information and cognitive processing environment that is already very complex and challenging.17,18 Viewed from this perspective, clinical nonresponse to reminders can be considered an adaptive response: actively filtering a stimulus that could produce a break-in-task event19 and hence disrupt the decision-making process for a patient's primary need.
Taking into consideration these concerns, the results of our cognitive task analysis, and the advice of our human factors engineer, we developed a set of 8 core principles to guide our design and implementation. These principles are listed in Table 1. Though the work by Patterson et al9 was not yet published as we were designing our intervention, our 8 principles converged independently on the need to address 6 of the 10 barriers to CRS implementation they documented (workload, time to remove inapplicable reminders, false alarms, training, ease-of-use issues, and administration benefiting more than providers from clinical reminder use). The team-oriented implementation approach also designed out the physician–nurse coordination issues that Saleem et al10 found impeded CRS operation. Finally, our principles also allowed us to reach independently an important conclusion from the major primary care improvement initiatives in the United Kingdom: Improvement targets should be chosen for clinical value, not to control costs.22
The system that resulted from this design process, called “ClinfoTracker,” has been described in detail elsewhere.23 The system was subsequently licensed by the University of Michigan in 2006 to a startup firm (Cielo MedSolutions, LLC) for commercialization, but it remained unchanged in daily use, supporting patient care throughout the study period. Figure 1 illustrates the printed version of the reminder form printed by the system and given to the care team in advance of each visit. The on-screen version appeared very similar, with the exception of the response options being radio buttons. It was available for the team's use as an ordinary web form; it was not embedded in the electronic medical record. At each visit the clinician and other team members updated the problem list (independent of billing diagnoses) and indicated their responses to reminders either on the paper form or on-screen. Whichever form was used was simply made available for use—there was no requirement to interact with it—and could be referred to whenever and as many times as the team members chose. The on-screen version became available in 2009 but was used by only 2 clinicians, although it was available to all. The paper form was always available, even to on-screen users, and was overwhelmingly preferred by clinicians.

Printed version of the reminder form.
The process of building support and buy-in was initiated through discussions of evidence-based quality goals at monthly physician meetings. Discussion among the physicians guided the selection and specific details of reminders. These 2 activities addressed the first and second implementation principles in Table 1. We addressed the fourth implementation principle using feedback received during the monthly meetings and negotiations with administrators. For example, the asthma action plan reminder was launched then deactivated based on feedback. We worked with clinic directors to allocate registered nurse time and to obtain training for registered nurses before relaunching the reminder. We also discovered during monthly meetings that sites were using the reminder forms in novel ways to facilitate communications among team members, and we actively encouraged them to continue (third implementation principle). After the launch, we began publicly recognizing physicians with high response rates at the monthly meetings (awarding first a coffee mug and subsequently gift cards for coffee). Finally, and only after most clinicians were regularly achieving high response rates, a small ($1 per relative value unit), individual quarterly payment incentive was implemented for achieving a 90% rate of documenting consideration of the problem lists and reminders issued at each visit, averaged over 3 months. All that was necessary to document consideration was return of the paper form or use of the electronic form with at least 1 item of data: a new or changed problem list entry, an existing problem checked as seen at this visit, or any response to any (not all) of the reminders. The incentive amounted to about $12 for a typical 4-hour clinic session.
The initial launch included only reminders for screening and prevention services selected by the physicians from among those recommended by the US Preventive Services Task Force. Once those were in use and the logistics of printing, distributing, collecting, and entering data from the paper forms in 5 offices were working smoothly, sets of reminders for chronic disease management were launched, 1 set at a time every 2 to 3 months. The sets requiring the most practice change and additional training and resources were launched last (heart failure and asthma). The full set was in place after a year. The full list of reminders is presented in Table 2.
Data Collection and Analysis
The data for these analyses were extracted from the CRS. All patient encounters between January 1, 2006 (when the CRS was first rolled out across all the sites), and July 31, 2012, were extracted. Encounters at which no reminders were issued were excluded. Our unit of analysis was an individual reminder issued during an office visit through printing on an encounter form. A reminder could be to perform a specific action (eg, administer influenza immunization) or to evaluate a clinical situation (eg, blood pressure is out of goal range, consider change in therapy). Response options included the following:
Done: taking the advised action during the visit (eg, administering influenza vaccine, evaluating antihypertensive regimen)
Ordered: completing an order for the action (eg, placing a mammography requisition)
Not Cand.: documenting noncandidate status (eg, the patient had a hysterectomy for benign disease and does not need Papanicolaou tests)
Declined: documenting that the patient declined
Discussed: documenting that the issue was discussed but no decision was made
Not Addr.: documenting that the matter was not addressed (eg, patient presenting in crisis, discussion of colorectal cancer screening was inappropriate)
Logistic regression adjusted for clustering by visit was used to model the odds of a reminder being addressed as a function of patient age (in integer years), sex, time (months) since CRS launch, number of reminders issued during the visit, and number of active problems on the patient's clinician-verified problem list (as a proxy for patient complexity). Modeling was conducted using Stata software version 10.1 (StataCorp, College Station, TX). Response options 1, 2, 3, and 4 above were designated as “actions” in response to reminders, and option 5 was designated “consideration.” Models were computed both for outcomes of action and action plus consideration.
Results
A total of 988,149 reminders were issued during 453,537 encounters for 81,959 patients during the sampling frame. Three or more reminders were issued at 139,835 of these encounters. The distribution of the number of reminders per visit is presented in Figure 2. The median number of chronic clinical problems at a visit was 3 (interquartile range, 1–3), and 10% of visits involved patients with ≥5 active chronic clinical problems. The age and sex distribution of the patient population is described in Table 3.

Number of encounters with varying numbers of reminders.
Action was taken in response to 60.1% of reminders, and consideration was documented in another 26.8%, for a total rate of 86.9% of reminders attended to. The odds ratios for action in response to reminders by months since CRS implementation, by number of reminders during an encounter, and by number of problems were 1.01, 1.17, and 1.01, respectively. Age had no practical effect (odds ratio, 1.001), but sex had a substantial effect: The odds of a reminder response among women versus men was 0.65. There was no practical interaction between sex and months since launch (odds ratio, 1.003). The same model computed for the combined outcome of action or consideration was almost identical. These odds ratios are highly statistically significant because of the large sample, but all except sex are minimally different from 1 (and all are in the opposite direction from reminder fatigue). In other words, there was no decline in response to reminders over time, no decline in odds of response as number of reminders increased within a visit, and no decline with increasing patient complexity. Table 4 presents the full results of the logistic model.
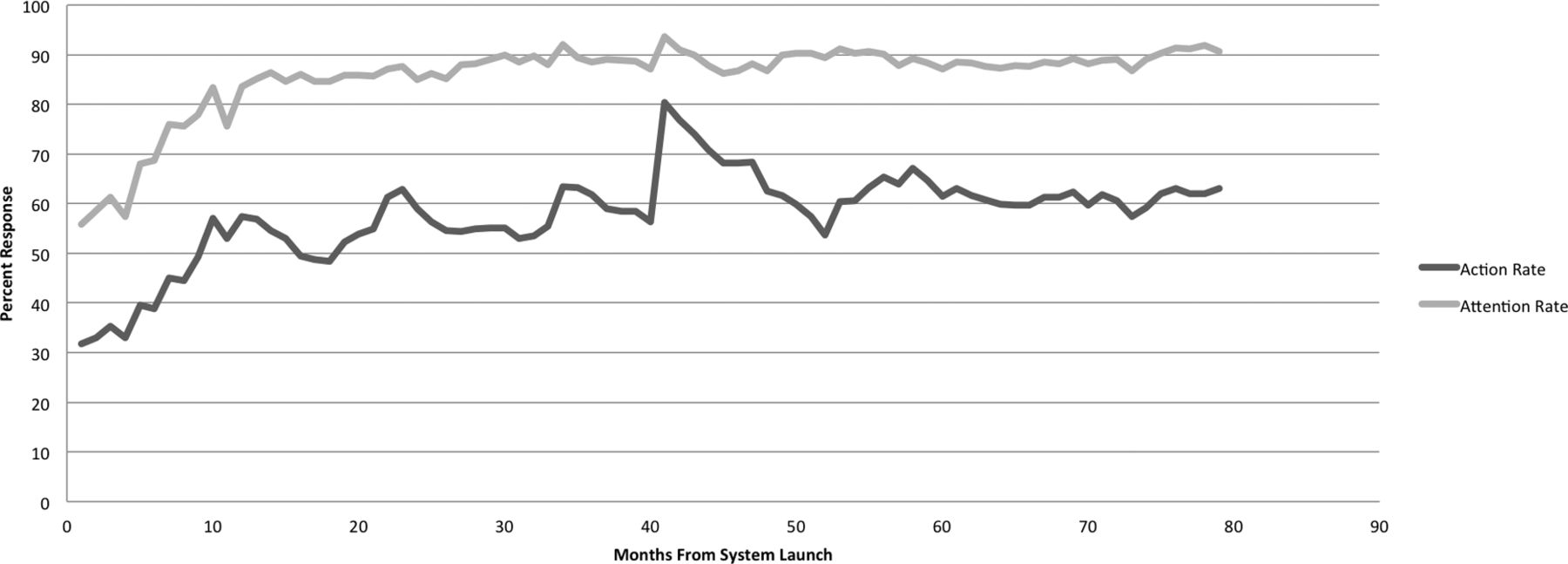
Figure 3 graphically illustrates the trends in reminder response (action taken and attended to) over time. The response rates rose steadily with the systematic implementation described, reaching a stable plateau with no evidence of reminder fatigue. Note that the seasonal spikes in action rates are the annual waves of influenza immunization; the largest is the H1N1 event.
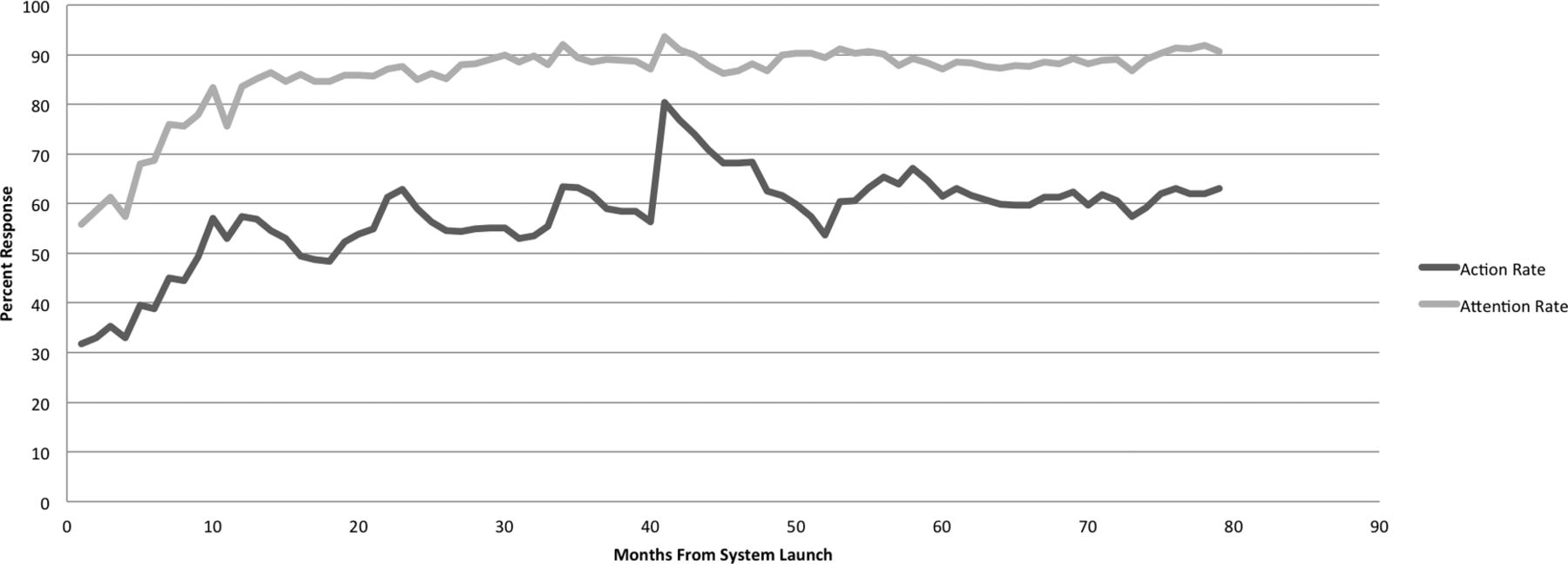
Reminder response rates by time.
Discussion
Our results demonstrate that reminder fatigue can be avoided by designing and implementing a CRS with careful consideration of current knowledge of cognitive science and human factors engineering. This example of a successful CRS is as notable for what is absent as for what is present: Our reminders include no information that does not need to be acted on, and information that can be accessed elsewhere is not duplicated. Patient history is left to the medical record, reference material is left to journals and online resources, and false positives are avoided through access to multiple sources of data behind the scenes. Our reminders prompt clinicians to act or consider only actions that they have already considered in depth through the process described in the Methods—and to prompt them as briefly and simply, as flexibly and nondisruptively, as possible.
One limitation of this study is that the principles enumerated in the Methods were applied as a package. We cannot state that any one of them was essential to the results achieved, estimate their individual contributions, or prioritize them. Comparing these results with those settings that have experienced fatigue is also difficult because in general they do not report in detail how they have applied the various methods noted above that might reduce fatigue. The importance of our results is not that they “prove” any particular component of the intervention, nor compare them with components that have been used elsewhere in the literature, but that they clearly demonstrate that reminder fatigue is not inevitable and document one way in which a CRS can be designed and implemented without suffering reminder fatigue. Other approaches could be possible as well. For example, we rigorously avoided the forcing function approach, but that approach has shown benefit in studies of medication safety prompting systems24,25 even though it also leads to high override rates.26 As another example, a recent Cochrane review1 found that computer-generated reminders delivered on paper were effective in changing practice and that providing space for physicians to respond led to greater effect size; including an explanation of the reminder, however, which we avoided, also improved effect size.
A second limitation is that this study was conducted in a single health system. While the 5 clinics varied widely in their patient populations, settings, and clinic workflows, all were part of a department with integrated leadership that became committed to the patient-centered medical home concept during the course of this project, and the implementation of this CRS was a core technology to support transition to the patient-centered medical home. The physicians were not selected for computer literacy, and some were notoriously not computer-oriented, but as members of an academic department they were a select group in terms of quality and team orientation.
It is also important to note carefully that this study demonstrates only that a CRS can achieve a relatively high and stable response rate without suffering from reminder fatigue. It is not a study of methods to improve response rates, nor a comparison of strategies to determine which yields less reminder fatigue. It is proof that a system can be designed and implemented such that response rates do not decline over time or with increasing numbers of reminders or visit complexity. It is, to the best of our knowledge, the only demonstration to date of an approach that yields no reminder fatigue.
Despite these limitations, our central finding is highly robust: In this setting, with this CRS implementation, reminder fatigue did not occur. We believe that these results are very consistent with our emerging understanding of the dual-process model of human decision making.27,28 Most clinical decision making is conducted in the “system 1” mode: rapid, recognition-based, and highly efficient in terms of cognitive effort. The “system 2” mechanism, deliberative reasoning, is slow and effortful and requires sustained attention. It is essential in addressing patients' primary concerns but can attend to only one task at a time. Distracting stimuli disrupt system 2 processing, and research in psychology has demonstrated the remarkable lengths to which our brains will go to filter out such stimuli when we are relying on system 2 to accomplish a task. In one famous experiment, >50% of participants failed to notice an actress in a gorilla suit walking through a scene thumping her chest while they were doing a task designed to require sustained system 2 attention to specific events occurring in the scene.29 Reminders that demand system 2 resources, such as those accompanied by a half screen full of explanatory and supporting text or that force attention at a time that disrupts active system 2 processing, such as sorting through a patient's complex set of presenting symptoms, will be filtered out in the saturated clinical environment. Attempts to overcome that filtering by stronger incentives, required responses, or other means of “turning up the volume” will not improve patient care, but only worsen the problem. Reminders carefully designed and implemented in such a way that they work with system 1 attention, that are familiar and easily processed, and that can be addressed when attention resources permit can avoid reminder fatigue effects. We believe that our CRS succeeded because it enabled clinicians to work effectively in system 1 mode most of the time or did not distract from clinical system 2 cognitive work.
Noting that this study used a CRS with an unusual degree of flexibility in both design and delivery of reminders is also important. That flexibility was not only with respect to physicians' use; the teams were able to allocate their roles and the options for responding among the team members as they saw fit. This flexibility contrasts with many electronic medical records, where basic design decisions are hard-coded into the software. Hard-coded CRSs are difficult to tailor to fit the workflow of individual users. They may not allow, or may price out of reach, the degree of end-user customization built in to the CRS used in this study, and they may demand system 2 processing on the part of clinicians. Avoiding reminder fatigue with the implementation of electronic medical records that cannot be flexibly tailored to fit the needs of end users may not be possible.
Conclusion
Our results demonstrate that using human factors and cognitive science principles to design a CRS to avoid reminder fatigue is possible. The highly variable results documented by various investigators examining the impact of electronic medical records on quality and improved patient outcomes illustrate the costly consequences of ignoring these principles. By incorporating these principles into future designs and versions of electronic record systems, the goals of improved quality and outcomes from electronic record adoption may be better realized.
Acknowledgments
The authors acknowledge the important contributions of programmer-analyst Timothy Morris, MA (deceased), coding and data entry specialist Norma Seimasz, and project specialist Kathleen Lambarth.
Notes
This article was externally peer reviewed.
Funding: This project was supported in part by the American Academy of Family Physicians.
Conflict of interest: DN served as the chief medical officer of the startup firm (Cielo MedSolutions, LLC), to which the University of Michigan licensed the technology developed in this project from 2006 to 2011. LAG and MSK served on the medical advisory board without compensation during that period. Cielo MedSolutions, LLC, was acquired by The Advisory Board Company, Inc. (ABCO) in February 2011. None of the authors are currently employed by or receive compensation from ABCO.
- Received for publication August 26, 2014.
- Revision received January 10, 2015.
- Accepted for publication January 28, 2015.




{kind=link}
{kind=link}
{kind=link}