
Abstract
Objective: In the Netherlands, general practitioners (GPs) and emergency departments (EDs) collaborate increasingly in what is called an Urgent Care Collaboration (UCC). In UCCs, GPs and EDs share 1 combined entrance and joint triage. The objective of this study was to determine if GPs treat a larger proportion of out-of-hours patients in the UCC system, and how this relates to patient characteristics.
Methods: This observational study compared patients treated within UCCs with patients treated in the usual care setting, that is, GPs and EDs operating separately. Data on the characteristics of the patients, their consultations, and their health problems were derived from electronic medical records. We performed χ2 tests, independent sample t tests, and multiple logistic regression analyses.
Results: A significantly higher proportion of patients attended their on-call GP within the UCC system. The proportion of ED patients was 22% smaller in UCCs compared to the usual care setting. Controlled for patient and health problem characteristics the difference remained statistically significant (OR=0.69; CI 0.66–0.72) but there were substantial differences between regions. Especially patients with trauma were treated more by general practitioners. Controlled for case mix, patients in the largest UCC-region were 1.2 times more likely to attend a GP than the reference group.
Conclusion: When GPs and EDs collaborate, GPs take a substantially higher proportion of all out-of-hours patients.
Out-of-hours emergency care in the Netherlands is provided by ambulant emergency services, emergency psychiatric departments, emergency departments (EDs), and general practitioners (GPs). In this article we focus on the latter 2 items: EDs and GPs. Emergency health care in the Netherlands is briefly described in the Box 1.
Emergency care in the Netherlands.
GPs take care of patients with urgent primary care needs. EDs are geared toward patients who urgently need specialized care or diagnostic tests. Ideally, both methods of care should complement each other. In daily practice, however, Dutch EDs have to deal with numerous patients who refer themselves. These amount to more than 40% of the total ED population.1,2 This seems appropriate from a patient's perspective, yet a large proportion of these demands could be managed by a GP or do not need urgent care at all. An international systematic review by Carret et al3 indicated that 20% to 40% of all ED consultations were inappropriate. In a Dutch study by Yzermans et al,4 21% of the ED contacts were labeled “inappropriate” by the emergency physician and 29% as “inappropriate but understandable.” In addition, Jaarsma-van Leeuwen et al1 determined the incidence of inappropriate ED attenders as 60%. This places a burden on emergency health care: It causes inappropriate use of services, high costs, and overcrowding,5,6 leading to lengthening queues and possibly lower standards of care.
Innovations
A few organizational innovations have been introduced to try to break through this status quo. These accept the challenge of organizing emergency care more efficiently while at the same time preserving its accessibility. Such innovations all require more collaboration between GPs and EDs.
One of the innovations being introduced is GPs working within EDs. Previous studies show that this innovation leads to reduced rates of medical examinations, therapeutic interventions, and hospital follow-up. It also seems to be cost-effective.7,8 A possible disadvantage of this innovation is that GPs who work directly within an ED may adjust their own medical practice to fit in with common ED practices. Westert9 showed that specialists choose different lengths of stay when working in different hospitals, thereby demonstrating that setting affects behavior.
Another option is greater collaboration between GPs and EDs within what we call an “urgent care collaboration” (UCC). Here, GPs and EDs each have their own department, while sharing 1 combined entrance and joint triage. In UCCs, patients are allocated to either the GP or the ED based on a system of triage. A possible advantage of this innovation is that, rather than GPs working within an ED, both parties preserve their own identity, philosophy, and specialism. GPs adhere to a philosophy with a greater focus on health promotion and a wait-and-see approach, whereas EDs are more medically focused and reliant on examinations and medical interventions. There is now a growing tendency toward implementing UCCs.10,11 This is intended to provide patients with the most suitable treatment and improve the efficiency of emergency care. Some evaluations and studies, though scarce, suggest that UCCs could improve efficiency in emergency care by encouraging a shift from EDs to GPs.12,13
There is a compelling need for studies of the effect of UCCs since little specific research has been carried out on this subject and information is still neither complete nor conclusive. This is particularly true given the growing tendency toward the cooperation or integration of EDs and GPs and encouragement by the Dutch government.
Hypotheses and Research Questions
In this study we chose to compare, during out-of-hours care, settings in which EDs and GPs work separately (predominantly the usual practice) with settings in which they collaborate within UCCs. We focused on out-of-hours care because the organizational model is different during normal working hours compared with out-of-hours care (see the Box 1).
We hypothesized that UCCs promote a substitution, or switch, of patient care from EDs to GPs and that this substitution is selective. This causes differences in the population characteristics of GPs and EDs in settings in which they work separately (ie, usual care) compared with UCCs. This study examined to what extent patients are treated more often by GPs in UCCs and how this relates to the characteristics of the patients, their consultations, and their health problems.
Methods
Study Design
An observational study was performed to compare settings in which GPs and EDs collaborate within UCCs with settings in which EDs and GPs work separately. We chose this type of study because the design does not require a random assignment of patients to an intervention or control group.
This study was conducted in 3 regions in which UCCs have been adopted and in 3 regions in which EDs and GPs work separately. All 6 regions are located in the southeastern part of the Netherlands.
Patients were sampled outside of normal working hours, that is, between 5:00 p.m. and 8:00 a.m. on working days and throughout the day on Saturdays, Sundays, and public holidays. Sampling was conducted between March and April 2011 and October and November 2011. These periods were determined a priori to rule out seasonal effects.
Settings: UCCs and Usual Care
The usual care group consisted of patients who attended a GP and/or an ED in the usual care setting in which both parties work separately but are located relatively close to each other (within 5 km). In this setting, patients may decide to contact a GP, by telephone if possible, resulting in medical advice about how the patient can take care of themselves. It may also lead to a consultation at the GP's practice or at the patient's home. If necessary, the GP refers patients to an ED. However, patients can also attend an ED directly. At GP practices participating in this study, triage is performed by a medical assistant (a health care professional who supports the work of a GP by performing routine tasks and procedures, triage, and patient scheduling) using the Netherlands Triage System.14 or Telephone Advice System. Within the EDs, triage is performed by nurses using the Manchester Triage System or the Emergency Severity Index. The latter two are the most frequently implemented 5-level triage systems in the Netherlands15 Triage is used to assign a level of urgency (very urgent [U1] to less urgent [U5]).
The UCC group consisted of patients who attended a GP or ED in an UCC setting. The UCCs participating in this study were launched between December 2008 and March 2009. The UCCs share a location and have 1 telephone number, and patients check in at a single joint reception. Based on a system of triage, patients are allocated to either a GP or an ED and are assigned a level of urgency. Health problems presented by telephone are triaged by a trained medical assistant. Health problems presented on site are triaged by a trained nurse. In both cases, the Netherlands Triage System14 is used. Within the UCCs, patients cannot decide for themselves whether to contact a GP or ED because they share a location, use joint triage, and share a single entrance. After triage, GPs and EDs each have their own department. A patient's treatment is similar to that received within a usual care setting. The main difference is how the care is allocated: to either a GP or an ED.
The UCC and the usual care groups are situated in both rural as well as urban areas. Both regions have comparable numbers of inhabitants (538,000 vs 533,000).
Data
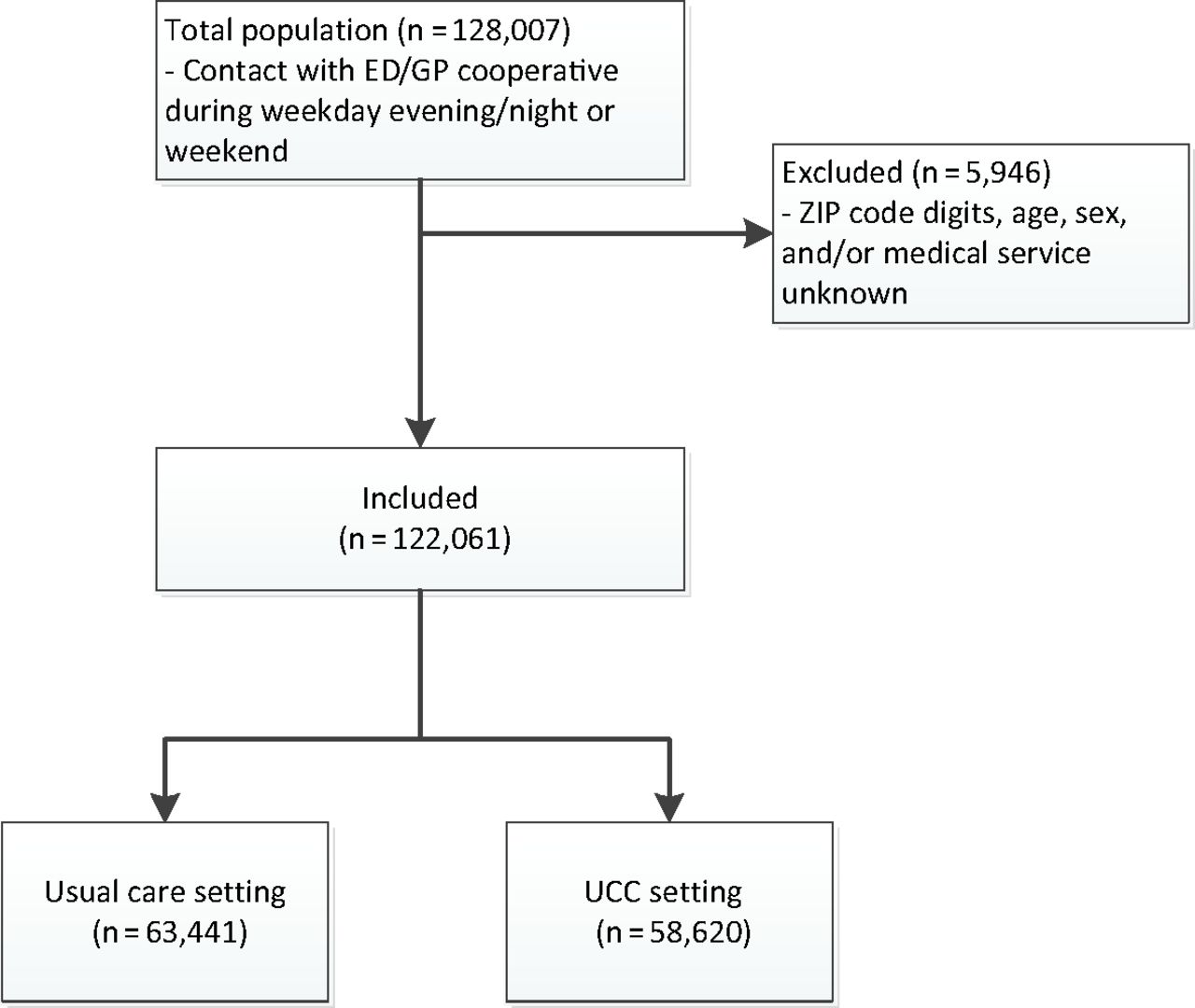
Data were obtained from electronic medical records for all patients who contacted a GP or ED during the sampling periods. For each telephone call or consultation, the relevant records were collected. Data included information about patient characteristics (sex, age); consultation characteristics (the medical service obtained, the moment of contact, region); and health problem characteristics (level of urgency and health problem). Cases that lacked ZIP code digits, patients age, patients sex, or data on the medical service obtained were excluded. In total, 5946 cases (4.6%) were excluded (see Figure 1).
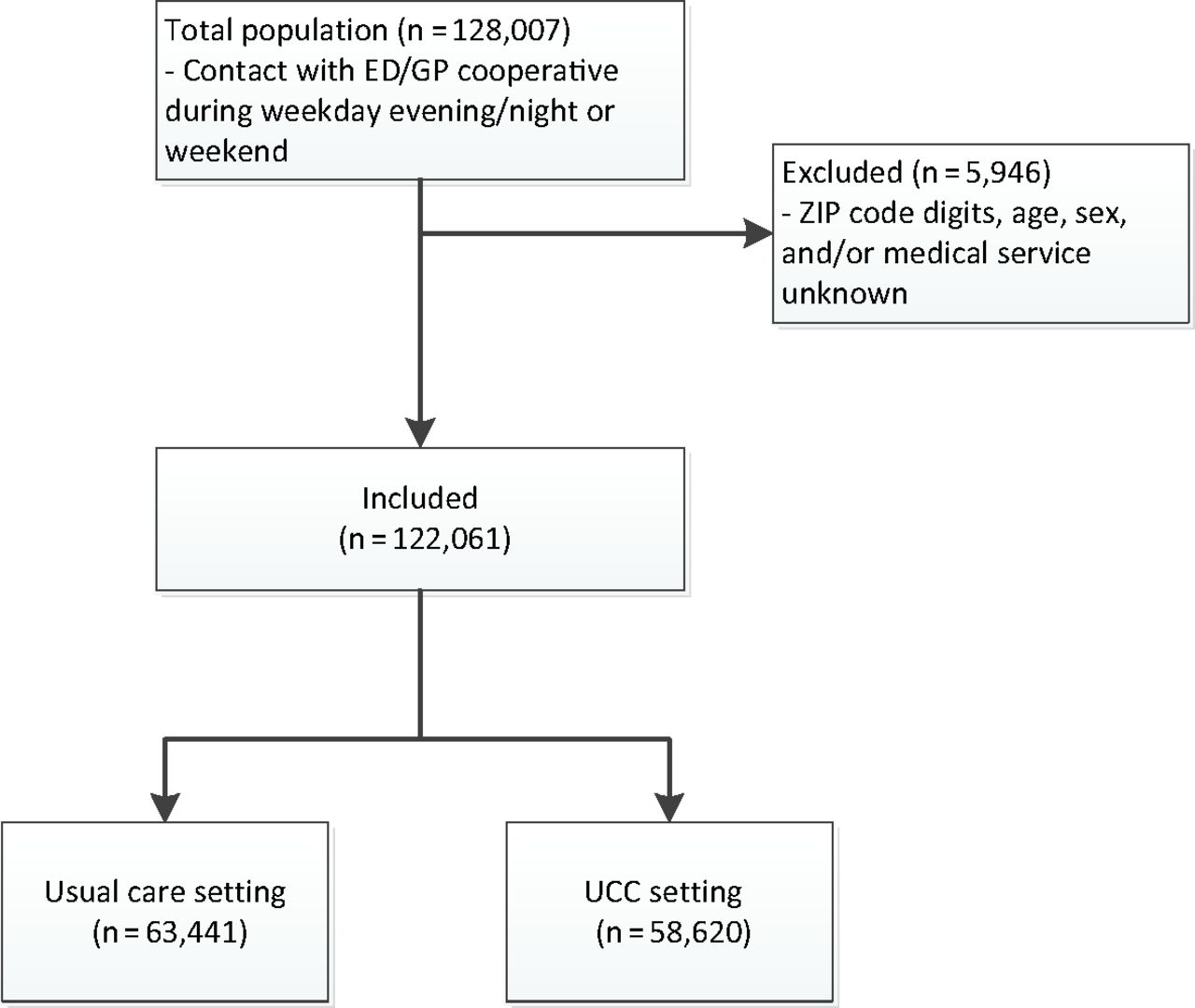
Study flow chart. ED, emergency department; GP, general practitioner; UCC, urgent care collaboration.
The 6 regions included in this study were assigned the letters A to F; A to C were the usual care settings and D to F were UCCs. Age groups were based on different stages of life: preschool (0–4 years), school age (5–14 years), adolescence (15–24 years), adulthood (25–44 years), middle age (45–64 years), aged (64–74 years), and very old age (>74 years). The medical service obtained was subdivided into 4 categories: medical advice from a GP, consultation at a GP practice, consultation with a GP at home, and treatment at an ED. The moment of contact corresponded to the moment of registration, which was either the time of the telephone call or check-in at the reception. The moment of contact was clustered into evening (Monday through Sunday, 5:00 to 11:00 p.m.), night (Monday through Sunday, 11:00 p.m. to 8:00 a.m.), and daytime (weekend or public holidays, 8:00 a.m. to 5:00 p.m.). The degree of urgency was one of the results obtained from the triage system and was obtained directly from the databases. It was reduced to 3 levels: very urgent (U1 and U2), medium urgency (U3), and less urgent (U4 and U5).
Health problems were registered using the International Classification of Primary Care (ICPC).16 GPs used ICPC coding to define health problems. However, they were able to skip ICPC coding and describe the health problem in a written note. In cases where the ICPC coding was missing (35.2% of all cases), trained medical students who had completed a Bachelor of Medicine degree encoded the health problem based on the aforementioned written note. EDs used diagnostic-treatment combinations (DTCs) to describe the health problem and treatment. A DTC consists of 4 aspects, including medical diagnosis. These diagnostic codes were converted to ICPC codes by a trained medical student. The ICPC codes were grouped in clusters arranged by the nature of the health problem rather than how the health problem relates to the patient's body4: acute somatic, infections, trauma, chronic or long-lasting diseases, and “other.” The cluster “trauma” comprised all health problems caused by physical harm from an external cause, varying from less severe to very severe.
Analysis
The variables were summarized separately for usual care and for UCCs using means and standard deviations for continuous variables. Numbers and percentages were used for categorical variables. A χ2 test was used to test whether the proportion of patients treated by the ED in the usual care setting differed to a statistically significant degree from the proportion treated in the UCC setting.
χ2 Tests were performed for categorical variables to test whether there was a difference in the number and characteristics of the patients who presented to GPs and EDs between usual care and the UCCs. The accompanying effect sizes (Cramer's V) were calculated. t Tests were used for continuous variables if the variables were normally distributed. If not, Mann-Whitney U tests were used. Logistic regression analysis was used to assess the association between setting or region and urgent care provider (GP or ED), controlled for case mix variables.
The data were analyzed using SPSS Statistics 20.0 (IBM, Chicago, IL). A 2-tailed P value <.05 was considered to be statistically significant. Effect sizes were interpreted as follows: small = 0.1, medium = 0.3, large = 0.5.
Results
Between March and April 2011, and October and November 2011, 128,007 patients contacted an ED or GP for out-of-hours care. Of these, 95% were included in this study (Figure 1).
Characteristics
The study population comprised 58,620 cases in the UCC group and 63,441 in the usual care group. Population characteristics are shown in Table 1. There were no relevant differences in patients sex and age between both settings.
Fewer Patients Attend EDs, More Patients Go to GPs
Within the UCC setting, 21.6% of all patients consulted an ED, whereas this was 27.6% in the usual care setting (Table 1). A χ2 test showed that this proportion was significantly lower in UCCs compared with the proportion in the usual care setting. In addition, the proportion of GP consultations at home (5.1% vs 6.1%) and the number of occasions when medical advice was given (29.5% vs 31.0%) were also smaller in the UCCs, whereas more people consulted a GP (43.8% vs 35.3%) at the UCCs.
Differences in Population Characteristics of GPs and EDs: UCCs versus Usual Care
A close examination of the population characteristics (Table 2) shows that less urgent cases presented more often to GPs (90.9% vs 85.1%) in UCCs compared with usual care. Moreover, it seems that UCC patients in the age groups comprising 5 to 64 years were treated relatively more often by a GP (mean, 79% vs 69%; V = 0.087) than their peers in the usual care setting. The effect sizes were largest for the age groups 5 to 14, 15 to 24, and 25 to 44 years (0.102 < V < 0.157). During all time frames, a relatively larger number of patients was seen by GPs in UCCs compared with usual care, yet the greatest difference occurred during evening hours (77.8% vs 70.2%; V = 0.087).
With regard to the clusters of health problems, the data revealed a difference between settings. In UCCs compared with usual care, it stands out that patients who presented with trauma were more often treated by a GP in UCCs compared with usual care (80.3% vs 62.0%; V = 0.200). When looking more closely at this cluster (Table 3), it seems that the GPs working in the UCC setting had to deal with more lacerations, sprains, strains, and burns—health problems that seem to be less severe. In UCCs, patients within the cluster “other” (16.1% vs 7.3%; V = 0.137) and “chronic or long-lasting diseases” (29.9% vs 24.4%; V = 0.061) were more often treated by the ED compared with usual care.
Case Mix Adjustment
Regression analysis (Table 4) showed that setting, both unadjusted and controlled for case mix variables, was significantly associated with the health care provider outcome. UCC patients were less likely to be treated at the ED than their peers in the usual care setting. When controlled for patient and health problem characteristics, the odds ratio (OR) for ED treatment was 0.691 (95% confidence interval [CI], 0.662–0.721) in the UCC setting.
UCCs exist within 3 regions; therefore we could replace setting with region in the regression model. The results showed that the effects differ per region. When controlled for patient and health problem characteristics, patients in regions B, C, and E were not more or less likely to attend an ED than the reference category (region D). However, the odds of being treated at an ED were significantly smaller in region A (OR, 0.826; 95% CI, 0.726–0.895) and significantly larger in region F (OR, 1.514; 95% CI, 1.407–1.629).
Discussion
To the best of our knowledge, this is the first study to describe in depth the substitution or shift of care from EDs to GPs as a result of UCCs. In other studies12,13 this substitution was handled superficially as a part of patient flow. Emergency health care in the Netherlands shows a trend toward more cooperation between EDs and GPs. This development is supported by government policy. However, thorough insights are necessary to guide national and international policymakers and to manage the consequences of such integration. We provide a new perspective on the effects of UCCs by describing the magnitude of the substitution and by characterizing the nature of this shift.
UCCs: Three Quarters of Patients Were Treated By GPs
Our study shows that a significantly lower proportion of patients attended the ED in UCCs: 21.6% as opposed to 27.6% in usual care. By extrapolating the data, this implies that UCCs can elicit a substitution of 21.6 contacts/1000 inhabitants a year, a substantial substitution. The number of ED patients was 22% smaller (6%/27.6%) in UCCs compared with the usual care setting.
In UCCs, GPs take care of more than three quarters of all patients. This implies that UCCs are effective in intercepting patients who attend the ED. Nevertheless, these numbers seem modest if compared with international figures of inappropriate ED contacts,3 which vary between 20% and 40%. This may be explained by 3 reasons. First, studies looking at patients attending health facilities inappropriately focused only on EDs and patients who inappropriately request specialized care. They did not take into account a possible backflow of patients who are entitled to ED care but do not request it.
Second, these studies were performed in different countries with different arrangements for out-of-hours care. A study by Schoen et al17 showed that 97% of Dutch GPs have out-of-hours arrangements for their patients to see a doctor without going to an ED. By contrast, this is <50% in Canada, Australia, Norway, and the United States.17 In addition, Villani and Mortensen18 discovered that difficulty in contacting one's usual source of care is associated with more unnecessary ED visits. If out-of-hours care is already being organized efficiently, only small improvements may be expected. When viewed from that perspective it seems that UCCs are a fine-tuning of an already well-functioning emergency care organization.
Third, triage may not be as objective as desired. It is possible that an “overtriage” occurs either when a patient's wishes are granted too easily or simply because the triage nurse prefers to err on the side of safety, thus preventing any danger of “undertriage.” Moreover, the triage nurse might tend to allocate patients to the ED precipitately because he or she might be more familiar with the ED since GPs work at UCCs only during out-of-hours care, or because he or she might be, to some extent, unfamiliar with the capability of the GP service.
Results Differ By Region
The regression analyses showed that regions A and F—the regions with the most patients—tower above the others in terms of visiting a GP or ED when controlled for the patient characteristics, their consultations, and their problems. Patients attending the UCC in region A are 1.2 times more likely to attend a GP than those in region D, whereas patients in region F are 1.5 times more likely to attend an ED.
Strengths and Limitations
A major strength of this study is that it was based on a large population, and sampling was conducted during 2 periods (the spring and autumn), which minimized seasonal influences and supported the degree to which we could make general conclusions. It also was improved by the selection of both rural and urban areas. Furthermore, the extensiveness of our study was also a major strength. While other studies of substitution from EDs to GPs mainly focus on self-referrals, this study comprised the ED and GP population in total. At the same time, the differences in patient characteristics were studied and factors associated with allocation to an ED or GP identified.
The limitations are, first, that all hospitals and GPs have their own registration system. This could lead to information bias, although we do not expect this. Second, the hospitals and GPs do not all use the same triage support system and have different backgrounds regarding triage. Therefore we cannot be sure that the levels of urgency relate to similar patients. Third, although the populations attending the UCCs and the GPs were large, the sample size of this study is limited: 3 UCC regions were compared with 3 usual care regions.
Implications for Further Research and Clinical Practice
A few UCCs are now established, and several GPs and EDs are exploring the possibility of either working more closely together or integrating entirely. The results of this study may support the discussion of the organization of out-of-hours emergency care. We suggest that future research should monitor the number of patients inappropriately attending EDs as well as GPs. This should be carried out for both over- and underattendance to determine more precisely how effective UCCs are in intercepting patients inappropriately attending one or the other service. Moreover, more extensive research on triage in UCCs is necessary.
Acknowledgments
The authors thank the staff of the hospitals and GP cooperatives for the invaluable contribution of their time and effort in participating in this study. The authors also thank the medical students who encoded the health problems (based on the ICPC), especially Ties Yzermans for converting all DTC diagnostic codes to ICPC codes. We are grateful to Harald Abrahamse for his help in preparing the data set and Lucas van der Hoek for all his statistical advice.
Notes
This article was externally peer reviewed.
Funding: This research was financed by ZonMW, The Netherlands Organisation for Health Research and Development, The Netherlands Institute for Health Services Research (NIVEL), the Scientific Centre for Transformation in Care and Welfare (Tranzo, Tilburg University), and the GP Cooperative Zuidoost Brabant.
Conflict of interest: ESJvG-vR performed this research as a science practitioner at Tranzo, Tilburg University. ESJvG-vR and GPW are employed by one of the study subjects.
- Received for publication September 4, 2014.
- Revision received July 1, 2015.
- Accepted for publication July 7, 2015.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Variation in daytime general practice services and association with out-of-hours use for older patients: protocol for a Danish cohort study
- Triaging and Referring In Adjacent General and Emergency Departments (the TRIAGE trial): a cluster randomised controlled trial
- Managing costs and access to healthcare in the Netherlands: impact on primary care
- What do we know about demand, use and outcomes in primary care out-of-hours services? A systematic scoping review of international literature
- The impact of general practitioners working in or alongside emergency departments: a rapid realist review
- New Tools and Approaches for Family Physicians