
Abstract
Background: The increasing number of community-dwelling frail elderly people poses a challenge to general practice. We evaluated the effectiveness of a general practitioner–led extensive, multicomponent program integrating cure, care, and welfare for the prevention of functional decline.
Methods: We performed a cluster controlled trial in 12 general practices in Nijmegen, the Netherlands. Community-dwelling frail elderly people aged ≥70 years were identified with the EASY-Care two-step older persons screening instrument. In 6 general practices, 287 frail elderly received care according to the CareWell primary care program. This consisted of proactive care planning, case management, medication reviews, and multidisciplinary team meetings with a general practitioner, practice and/or community nurse, elderly care physician, and social worker. In another 6 general practices, 249 participants received care as usual. The primary outcome was independence in functioning during (instrumental) activities of daily living (Katz-15 index). Secondary outcomes were quality of life [EuroQol (EQ5D+C) instrument], mental health and health-related social functioning (36-item RAND Short Form survey instrument), institutionalization, hospitalization, and mortality. Outcomes were assessed at baseline and at 12 months, and were analyzed with linear mixed-model analyses.
Results: A total of 204 participants (71.1%) in the intervention group and 165 participants (66.3%) in the control group completed the study. No differences between groups regarding independence in functioning and secondary outcomes were found.
Conclusion: We found no evidence for the effectiveness of a multifaceted integrated care program in the prevention of adverse outcomes in community-dwelling frail elderly people. Large-scale implementation of this program is not advocated.
- Aging
- Delivery of Health Care
- Frail Elderly
- Geriatrics
- Geriatric Assessment
- Interdisciplinary Health Team
- Primary Health Care
Population aging has a profound effect on the number of frail elders and is a major challenge for health care systems. Frailty is a condition in which losses in several domains of functioning lead to a declining reserve capacity and a subsequently increased vulnerability in functional decline, dependence, hospitalization, institutionalization, and death.1⇓–3 It is thought to be present in up to a quarter of people aged ≥85 years.4 The complex and interacting health care needs of these frail elders can be addressed only in a system that integrates health care and welfare services. This approach is supposed to delay the onset and progression of frailty and prevent its adverse outcomes, including functional dependence and institutionalization.5
In countries with a strong primary care system, such as the Netherlands, general practitioners (GPs) provide continuous, person-centered care to community-dwelling frail elderly people. Care delivery is facilitated by the use of high-standard electronic medical records (EMRs) and patient panels, defining the population under care.6,7 In the Netherlands, GPs often collaborate with practice nurses in the delivery of care (programs) according to the needs of the practice population.7 Moreover, physicians providing geriatric care increasingly operate (as consultants) in caring for frail older people in the community.8 However, the coordination between GPs, other primary and specialist care providers, and home care and community services is often perceived to be insufficient, leading to fragmented delivery of care.9 Many opinion leaders therefore plea for a redesign of primary care services for frail elders.
In the past 20 years, this perceived need has led to the development of several integrated care programs targeting frail elderly people. Systematic reviews have shown these programs to vary considerably in content, the disciplines involved, intensity, duration, and setting. These studies have shown no or merely modest and inconsistent effects on clinical outcomes and health care utilization,10⇓–12 which is disappointing. To date, therefore, there is no conclusive evidence for an efficient and effective approach to redesigning geriatric primary care. In addition to the need for coordinated and integrated care, the need for medication intervention programs aimed at the management of polypharmacy (ie, the [over]use of multiple medications) is widely recognized.13⇓⇓–16
In Dutch primary care this has led to a well-supported belief that community-based geriatric care needs to be multifaceted, combining structured multidisciplinary collaboration between professionals from cure, care, and welfare domains; proactive care planning; case management; and medication review.17 Therefore we designed the CareWell primary care program, which combines the above elements and aims for the prevention of functional decline, maintenance of well-being, and prevention of institutionalization and hospitalization among community-dwelling frail elders. This article reports the results of the cluster controlled effectiveness trial.
Methods
We conducted a 2-arm, nonrandomized, cluster controlled trial in primary care in the municipality of Nijmegen, the Netherlands, between September 2011 and September 2012. To prevent contamination bias, we used a cluster controlled design with allocation by GP practice.18,19 Details were published previously.20 The study was reviewed by the ethics committee of the Radboud University Medical Centre Nijmegen (registration no. 2010/403) and registered at ClinicalTrials.gov (identifier NCT01499797).
Recruitment
Eligibility criteria for GP practices were (1) a sufficient number of patients aged ≥70 years on their patient list, (2) adequate practice facilities enabling (future) implementation of the program, and—in the intervention group—(3) a solid motivation to adopt the program to reach optimal implementation. Six eligible GP practices were recruited for participation in the intervention arm and were informed about the program. Then, 6 GP practices were recruited for the control group without being informed about the program. They were explicitly asked to deliver “care as usual” and to decline new relevant interprofessional collaborations during the intervention period. No restrictions were imposed on preexisting collaborations between GPs and (practice) nurses.
GPs in both arms were trained to apply the concept of frailty and to identify study participants using the EASY-Care Two-Step Older Persons Screening (TOS) instrument.21 The EASY-Care TOS has shown good construct validity and interrater reliability, and is well accepted by primary care professionals.22,23 All practices were instructed to include 50 frail elders aged ≥70 years. Exclusion criteria were admission to a residential or nursing home and/or critical or terminal illness. After the Easy-Care TOS assessment, the GP and practice nurse/research assistant made a final decision on the presence of frailty, based on clinical reasoning using all explicit and tacit information.21 In addition, the complexity of the care context, representing the organization and coordination of care, was judged.24 Frail elders with and without complex care were included. Details on the recruitment of practices and participants have been reported previously.20
Intervention
The CareWell primary care program consisted of 4 key elements: multidisciplinary team meetings, proactive care planning, case management, and medication review.
Each practice assembled a core multidisciplinary team consisting of the GP, the practice nurse (or, if unavailable, a community nurse), an elderly care physician (ECP)8, added to the team to secure geriatric expertise and knowledge on proactive care planning, and a social worker with expertise on social and welfare domains. No structural collaborations between GPs, ECPs, and social workers were readily available at the time of the intervention. Team meetings were held every 4 to 8 weeks. In addition, team members were able to communicate virtually through a secure, Web-based health and welfare information portal.25
Proactive, individually tailored care plans were formulated for each participant upon enrollment in the program; these plans were based on individual health-related goals and needs as assessed with the EASY-Care TOS. Care plans were revised during the team meetings at least every 6 months and stored in the information portal.
A case manager (either a nurse or social worker) was assigned to each participant. Case managers were responsible for the planning and logistics regarding the team meetings and for coordinating and monitoring care. Furthermore, they were instructed to ensure participants' acknowledgment of the care plans, encourage their involvement in setting goals, and actively maintain treatment contact with the participants (and their informal caregivers) by telephone or home visits at least twice a year.
For each participant using ≥5 chronically prescribed drugs, a yearly medication review was held by the GP, the nurse, and a pharmacist.
In addition, we developed multidisciplinary guidelines for 8 common geriatric syndromes, a guideline on advance care planning, procedure agreements for easy-to-access consultation by geriatric experts, and procedure agreements between primary and specialized care providers upon hospitalization and discharge.20
Outcome Measurements
Common baseline characteristics of the participants were expanded with a socioeconomic status score, a cognition score, and a frailty index. The socioeconomic status score was based on postal code areas and calculated based on income, employment, and education.26 A cognition score was based on a modified Mini-Mental State Examination.22 The frailty index was defined as the proportion of accumulated deficits.22,27 All baseline characteristics were included in the EASY-Care TOS step 2. Furthermore, the items constructing the primary and secondary outcomes were enclosed. Data were collected at baseline and after 12 months through a home visit by either a trained nurse (in the intervention arm) or a research assistant (in the control arm). Outcome assessors were blinded to previous measurements but, for pragmatic reasons, not to the intervention arm. Additional health care utilization data were extracted from the EMR at follow-up.
Independence in functioning in (instrumental) activities of daily living, measured with the validated Katz-15 index,28 was used as the primary participants' outcome. Quality of life [measured with the EuroQol (EQ-5D+C) instrument],29 mental health (measured with the 36-item RAND Short Form Survey [RAND-36]),30 health-related social functioning (measured with 1 question that was based on the social functioning subscale of the RAND-36),30 institutionalization, hospitalization, and mortality were chosen as secondary outcomes.
Sample Size Calculation
Based on a power of 80%, a 2-sided α of 0.05, an assumed intracluster correlation coefficient (ICC) of 0.01,31 and an expected loss to follow-up of 35%, we calculated that we would be able to detect a clinically sufficient effect size of >0.32 on the Katz-15 index by including 50 participants from each of the 12 GP practices (total N = 600, assuming equal cluster sizes). Extended information on the sample size calculation was published in the study protocol.20
Statistical Analysis
Outcomes at the participants' level were analyzed with linear mixed-model analyses to account for the clustering of participants within the GP practices. Outcome estimates were corrected for significant differences in baseline characteristics that correlated with the primary outcome, and for the baseline value of the outcome (in the case of secondary outcomes) by including these variables as covariates. Subgroup analyses compared outcome estimates for participants in the lowest, middle, and highest tertiles of age and Katz-15 index scores, and for participants with and without complex care.
Residential and nursing home admissions, hospital admissions, and mortality were analyzed with binary logistic regression with correction for baseline values of the Katz-15 index. In evaluating admissions and mortality, no correction for baseline characteristics and covariates was done, since the number of events was too small to perform a multilevel analysis and the calculated ICC was found to be negligibly low.
Baseline differences were analyzed using t tests and χ2 tests. Tests were considered significant at P < .05. All statistical analyses were performed using SPSS software version 20 (IBM, Chicago, IL).
Results
Sample Characteristics
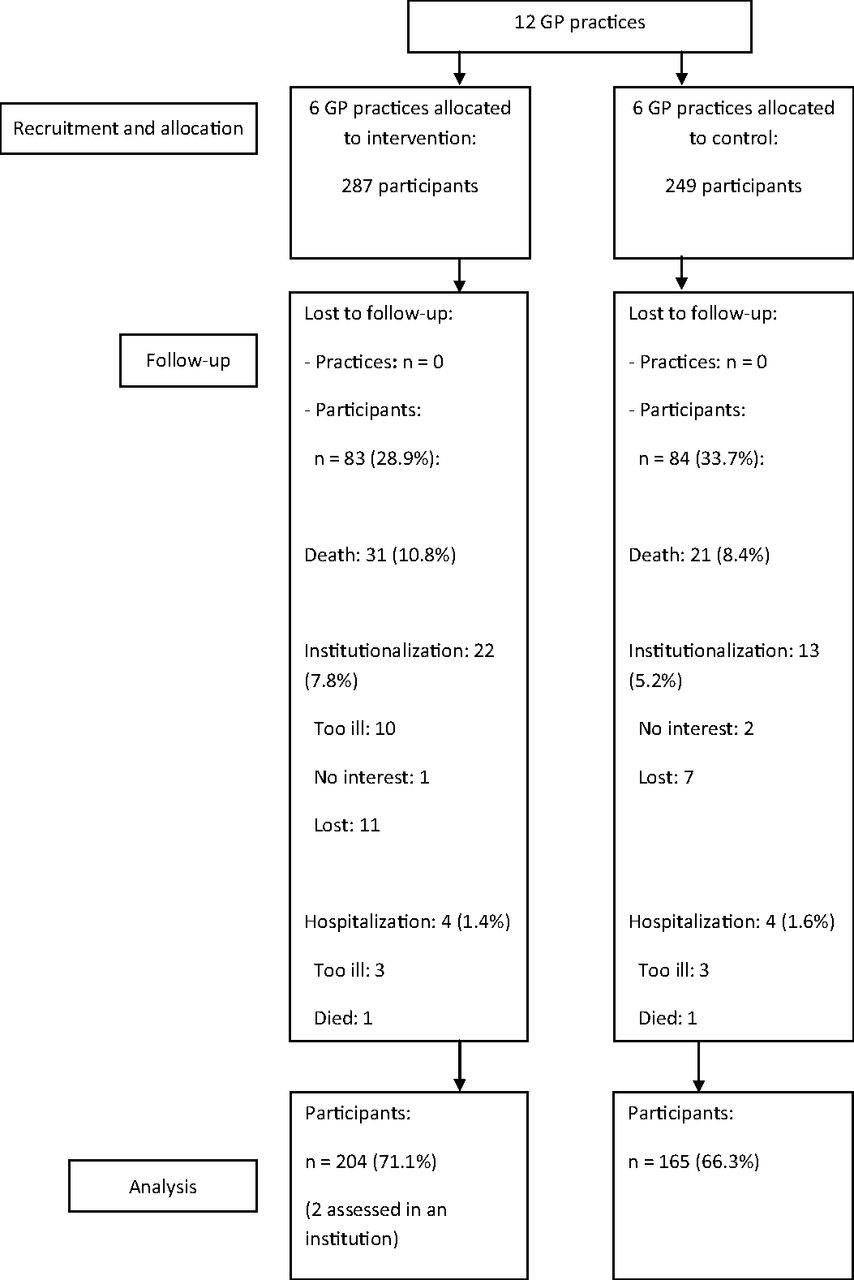
We included 536 participants: 287 in the intervention group and 249 in the control group. Baseline characteristics are shown in Table 1. Participants in the intervention group more often lived alone, had more health-related limitations in social functioning, more cognitive deficits, and more social disadvantage, and showed less complex care. These 5 characteristics correlated to the Katz-15 index score and were therefore used as covariates in our analyses. Furthermore, participants in the intervention group were higher educated.
We lost to follow-up 83 participants (28.9%) in the intervention group and 84 (33.7%) in the control group (Figure 1). The follow-up measurements therefore included 204 participants (71.1%) in the intervention group and 165 (66.3%) in the control group. Participants lost to follow-up in the intervention group were significantly older, more dependent in daily life, had more health-related limitations in social functioning, more cognitive deficits, more social disadvantage, and a more frail status, and were more educated compared with participants who were lost to follow-up in the control group.

Flow diagram of practices and participants. GP, general practitioner.
Patient Outcomes
The Katz-15 index score showed a greater increase, indicating more decline in functioning, in the intervention group compared with the control group. After correcting for clustering (with a calculated ICC of 0.05), relevant covariates, and the Katz-15 index score at baseline, no significant effects on functioning were found (Table 2). Moreover, we found no significant effects on quality of life, mental health, and health-related limitations in social functioning (Table 2). Subgroup analyses showed no mediating effects of age (divided into tertiles: <80, 80–85, >85 years); baseline Katz-15 index scores (divided into tertiles; <3, 3–6, >6); and the absence or presence of complex care, with the exception of small estimated intervention effects on quality of life (−0.18 (95% CI −0.36 to −0.00; P = 0.048) and on social functioning (0.29 (95% CI 0.10 to 0.48; P = 0.003) in the 80–85 year-olds in favor of the control group (data not shown in tables). No differences in residential and nursing home admissions, hospital admissions, and mortality were found (Table 3).
Discussion
We found no effects of the CareWell primary care program on functioning, quality of life, mental health, health-related social functioning, institutionalization, hospitalization, and mortality among community-dwelling frail elderly people in Dutch primary care. A strength of this study is the inclusion of a large sample of frail elderly people well defined by professionals who were trained in the concept of frailty. In addition, the inclusion of motivated primary care professionals in the intervention group and the use of several tailored implementation strategies supported the optimal implementation and benefit of the program. The implementation of the program in everyday practice contributed to its external validity.
We also consider some weaknesses. First, significant baseline differences existed between the study groups. These may have resulted from the cluster design that was used to prevent the spillover of intervention effects.19 Moreover, differences in the appraisal of participants' frailty by the GPs in both groups may have contributed. However, all professionals were trained in the concept of frailty and the use of the EASY-Care TOS to minimize these kinds of imbalances. Although we corrected for baseline differences, they may still have affected our results. Second, the allocation of motivated professionals to the intervention group might have led to differences in the quality of care delivery between groups in favor of the intervention group. However, since we found no between-group differences in effects on functioning and secondary outcomes, it is unlikely that the allocation procedure led to bias in favor of the intervention. Professionals in both groups used the EasyCare-TOS instrument, which may have led to “enhanced” usual care in the control group.32 We tried to minimize this effect by instructing the control practices not to start new activities related to the intervention, such as improved collaboration, making care plans, and starting medication reviews during the study period. Third, outcome assessors were not blinded to the intervention since this was not feasible. Last, participants with the least degree of functioning (ie, higher Katz-15 index scores) were more often lost to follow-up in the intervention group. However, since we assume that these participants would have the least potential to benefit, an effect in favor of the intervention group without this loss to follow-up is unlikely.
In the past 20 years, several studies have been conducted with programs targeting improving functioning and preventing institutionalization and hospitalization in community-dwelling frail elderly people. These studies have heterogeneous designs and settings and have yielded inconsistent results.10⇓–12 For example, Bernabei et al33 showed that an integrated community care program with standardized multidisciplinary meetings between the GP, nurse, geriatrician, and social worker reduced functional decline, institutionalization, and hospitalization. However, a home-based care management program delivered by a nurse and a social worker in collaboration with a geriatric multidisciplinary team, complementary to care delivered by the GP, showed no effects on functioning.34 More recently, Metzelthin et al35 found no effect on disability after introducing a program based on meetings between the GP and practice nurse, care planning, and regular monitoring and follow-up. Despite our efforts to optimally implement a fully integrated care and welfare program, we found no evidence for the effectiveness of this program in the prevention of functional decline, institutionalization, or hospitalization.
In addition to the methodological drawbacks, there are some other potential explanations for the absence of effects of the CareWell primary care program. First, the outcome measures used might not be specific and responsive enough in our targeted population. Although the Katz-15 index is applied in the vast majority of studies of functional decline and reliably predicts adverse health outcomes among community-dwelling frail elderly people,36,37 it might not be responsive to change in individual elders within a limited time span. Moreover, the EASY-Care TOS instrument identifies health risks related to functioning as well as to psychosocial and environmental domains that are negatively influenced by frailty. Subsequently, the programs' interventions and goals are highly individualized and heterogeneous. Outcome measures that are more person- and goal-centered (eg, goal-attainment scaling) might better measure the effectiveness of our intervention.38 Second, it is widely recognized that complex interventions are often not delivered or adhered to as intended,39⇓–41 which we accept as part of the outcome given the pragmatic nature of our study. Moreover, the follow-up period of 12 months may be too short to establish effective multidisciplinary collaborations, a true transition toward integrated care,41 and to achieve measurable effects on patient outcomes. A third explanation may be that the targeted population was too frail for the interventions to be effective in preventing adverse health outcomes. On the other hand, frail elderly people may appraise the boundaries of functional decline differently, leading to a willingness to adhere to preventive interventions at too late a stage, leading to low adherence at the participant level. A last explanation relates to the Dutch health care system, in which the GP already has a strong position and a central role in delivering geriatric care, often in collaboration with practice nurses, and facilitated by high-quality EMRs.7 This suggests that limited room for improvement exists in comparison to health care settings in which primary care is less well organized. On the other hand, our results may hold external validity to health care settings in which collaboration can be set up between health care and welfare and between primary and geriatric care.
Conclusion
We found no beneficial effects of our CareWell primary care program among community-dwelling frail elderly people in Dutch primary care. Current evidence is insufficient to advocate large-scale implementation of this multicomponent integrated primary care program. Further (longitudinal) studies are needed on the different trajectories of frailty and the most efficient timing of interventions. Moreover, research is needed on the validity and applicability of goal-oriented outcome measures in the field of geriatric research.
Acknowledgments
The authors are grateful to all participants and health care professionals who were involved in the study. Furthermore, the authors thank all professionals, volunteers, and health care organizations that are involved in Netwerk 100 (http://www.netwerk100.nl) for their contributions to the development of the CareWell primary care program.
Notes
This article was externally peer reviewed.
Funding: This trial was funded by the Dutch National Care for the Elderly Program, as initiated by the Netherlands Organization for Health Research and Development (ZonMW project no. 313050201). Health insurance companies (CZ and UVIT) and the municipality provided additional funding.
Conflict of interest: none declared.
Disclaimer: The funders had no influence on the analysis and reporting of the study.
- Received for publication July 8, 2015.
- Revision received October 7, 2015.
- Accepted for publication October 12, 2015.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Personalised care planning for older people with frailty: a review of factors influencing implementation
- Understanding the implementation of interventions to improve the management of frailty in primary care: a rapid realist review
- What long-term care interventions have been published between 2010 and 2020? Results of a WHO scoping review identifying long-term care interventions for older people around the world
- Use of standardized brief geriatric evaluation compared with routine care in general practice for preventing functional decline: a pragmatic cluster-randomized trial
- Cross-sectional study evaluating the association between integrated care and health-related quality of life (HRQOL) in Dutch primary care
- Frailty assessment in primary health care and its association with unplanned secondary care use: a rapid review
- Outcomes of Health System Structures, Highly Pertinent Clinical Information, Idea Stimulators, Clinical Reviews, and Prediction Tools: JABFM Exemplified