
Abstract
Introduction: Collaborative goal setting and action-planning are key elements of self-management support for people with type 2 diabetes mellitus (T2DM), however little is known regarding action plan quality or correlation of quality in primary T2DM care.
Methods: T2DM patients from 12 primary care sites participated in either: Connection to Health (CTH; 6 practices), consisting of a health survey followed by collaborative action planning, or Enhanced Engagement CTH (EE-CTH; 6 practices), including additional training in relationship building promoting patient engagement. Action plan quality was rated using an adapted version of the Goal-Setting Evaluation Tool for Diabetes (GET-D) (dual coding of 20%, inter-rater reliability [IRR] >80%). Associations with patient characteristics were examined using generalized linear mixed models adjusting for clustering by clinic and intervention arm.
Results: With a mean score ± standard deviation (SD) of 14.62 ± 3.87 on a 0 to 20 scale (n = 725), overall action plan quality was moderate-high. Higher health literacy (β = 1.184, 95% CI, 0.326–2.041; P = .007), and having no social risks (β = 0.416; 95% CI, 0.062–0.770; P = .021) were associated with higher action plan quality, whereas sex, age, language, education level, depression, stress, and health distress were unrelated to quality (P value not significant). Higher quality was associated with greater patient confidence in the plan (β = 0.050; 95% CI, 0.016–0.084, P = .004).
Conclusions: Although there was a considerable difference in action plan quality ratings, ratings did not systematically differ based on most patient demographic or mental health measures. Results suggest that action planning should be tailored to health literacy and social risks. Further research should examine associations between quality and longer-term clinical outcomes.
- Chronic Disease
- Disease Management
- Health Literacy
- Health Surveys
- Patient Participation
- Patient-Centered Care
- Patient-Reported Outcome Measures
- Primary Health Care
- Self-Management
- Type 2 Diabetes Mellitus
Introduction
Diabetes management is complex and relies heavily on developing patients' self-management skills since less than 1% of the patient's time is spent with a health care professional.1 The Patient-Centered Medical Home (PCMH) and Chronic Care Model (CCM) provide complementary frameworks that highlight the importance of active, personalized Self-Management Support (SMS) to improve patient outcomes.2⇓⇓⇓–6 Up to 95% of the variation in diabetes outcomes result from disease-related behaviors that require self-management.7 A person with diabetes (PWD) must learn to attend to a healthy diet, regular exercise, and an often complex medication regime, while simultaneously coping with common diabetes and non-diabetes-related stresses and psychological comorbidities, such as depression symptoms.8⇓–10 Self-management support (SMS) is a necessary part of diabetes care,4,11 with collaborative goal setting and specific short-term action-planning serving as key elements of SMS and key tenets of primary care quality improvement.1,4,12⇓–14 Primary care-based programs focused on goal setting and action planning have been linked in multiple studies with improved outcomes for diabetes, including decreases in HbA1c and increases in medication-taking and positive lifestyle changes.15⇓⇓–18 Although goal setting and action planning have been viewed favorably by clinicians in primary care,19 little is known about the quality of action plans created. This current gap in our knowledge constrains building knowledge around how best to identify important action plan components and where greater support or tailoring of care is needed.
To be effective, SMS can not be a “1-size-fits-all” approach.20 To deliver person-centered care the provider needs to be aware of the patient's greater daily life context and goals in conjunction with treatment plans.8,21 This includes how they are feeling (eg, diabetes distress and depression), their cognitive capacities, as well as social risks (eg, food, housing), and other life circumstances that can affect their capacity to engage in action-planning and behavior change.14,22 Validated patient-reported outcome (PRO) measures provide a systematic way to collect this information, and when used appropriately, have been shown to increase the focus on the PWD in clinical consultations and act as a decision support tool for clinicians.21 Understanding the extent to which patient characteristics and aspects of their life context are associated with action-planning can help identify crucial indicators for the provider to attend to before or while building these plans with individual patients to strengthen SMS delivery. For example, if depression symptoms are associated with low-quality action planning, then addressing depression either before or as part of the action planning process may be important. If low health literacy is associated with low-quality action plans, the approach to action planning may need to be adjusted for the patient to benefit from it.23
Connection to Health (CTH) and enhanced engagement CTH (EE-CTH) are 2 versions of an electronic tool created to facilitate SMS at the point of care in underserved or under-resourced primary care settings, to develop effective patient-centered action plans, and associated with decreasing in HbA1c in previous research.15 The program collects a comprehensive set of PROs through a health survey and guides providers and the PWD through a process of reviewing the PRO data, goal setting, and collaborative action planning. The action plans focus on a goal collaboratively selected by the PWD and their health care provider.1
The aims of the current study were to (1) assess the quality of action plans created in primary diabetes care across twelve Community Health Centers (CHCs) and to assess the extent to which these differ based on patient demographic factors (sex, age, language, race, educational level, and health literacy) and PROs related to life context (depression symptoms, general life stress, health-distress, and social risk factors (eg, food insecurity); and (2) examine the associations between action plan quality, patient demographic factors, and PROs with PWDs' perceived confidence in carrying out their action plan.
Methods
Design
This study includes PROs and action plans created in type 2 diabetes mellitus (T2DM) primary care visits as part of a 12-month 2-arm, pragmatic, cluster-randomized controlled trial designed to estimate the effect of implementing 2 versions of the CTH electronic program (CTH and EE-CTH), in CHCs. Both programs included an assessment of patient characteristics and PROs followed by either a focus on management-change action planning (CTH) or enhanced engagement (EE-CTH) action planning.
Sample
Twelve primary care CHCs in the San Francisco Bay Area were cluster randomized into the 2 arms of the study (6 practices each). Randomization was based on health system membership and T2DM panel size using a balancing criterion; with 1 randomization solution selected at random from the array of balanced randomization solutions.24⇓⇓⇓–28 Twelve clinical sites were enrolled from 5 safety-net health systems within the San Francisco Bay Area Collaborative Research Network29 (10 sites from 4 federally qualified health centers and 2 sites from 1 county health system). The clinics were responsible for the enrollment of eligible patients and the delivery of the CTH/EE-CTH programs using existing staff and providers with workflows modified as needed by the clinics to include the program elements. Patients were 18 years or older, diagnosed with T2DM, and receiving care at the clinic for 12 months or more before enrollment, and able to read in English or Spanish (greater than a sixth-grade level). The program was available in English and Spanish. Exclusion criteria included those with severe mental or cognitive disorders. Data for this study were collected between 2017 to 2020 and analyzed from 2019 to 2020.
Procedure
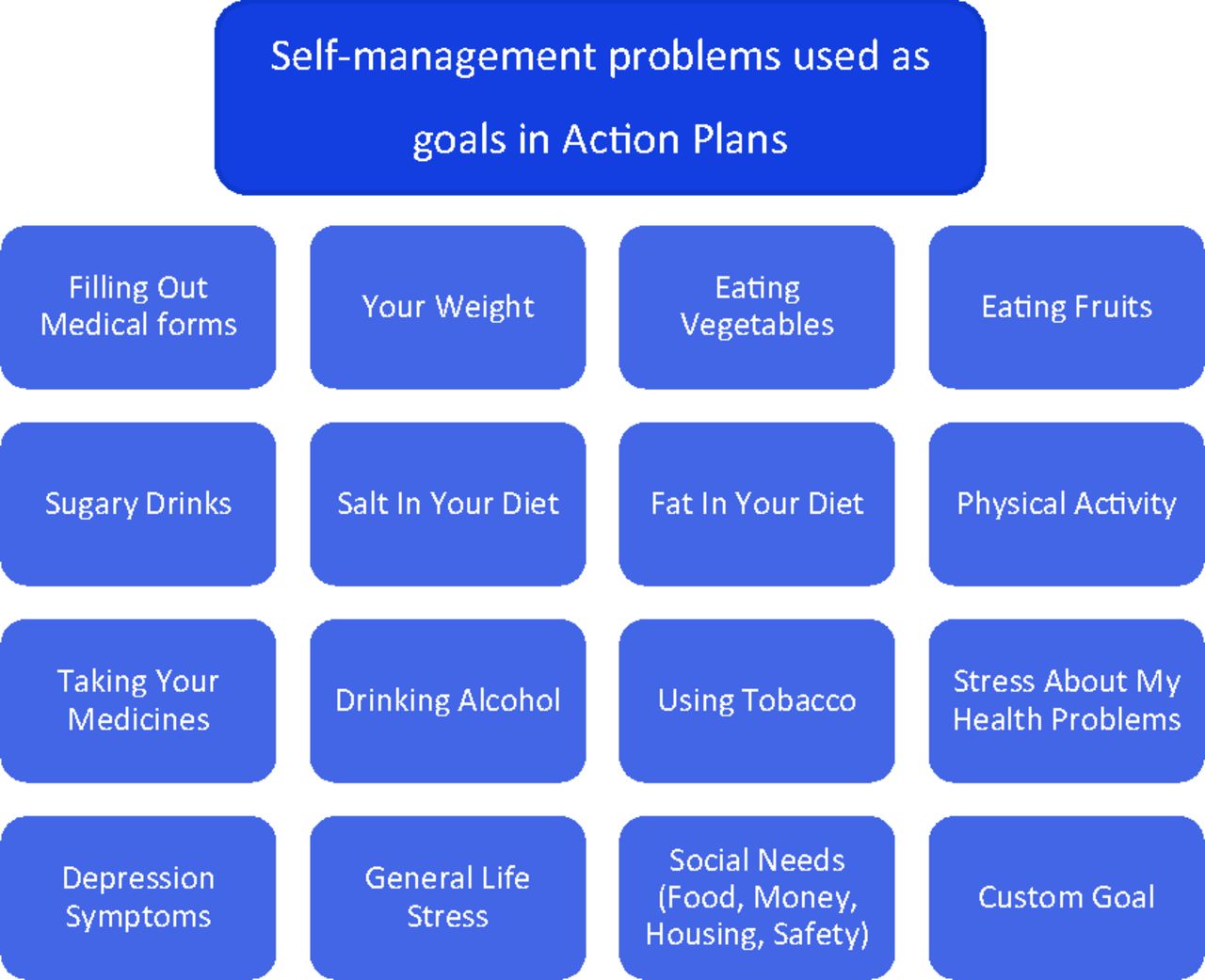
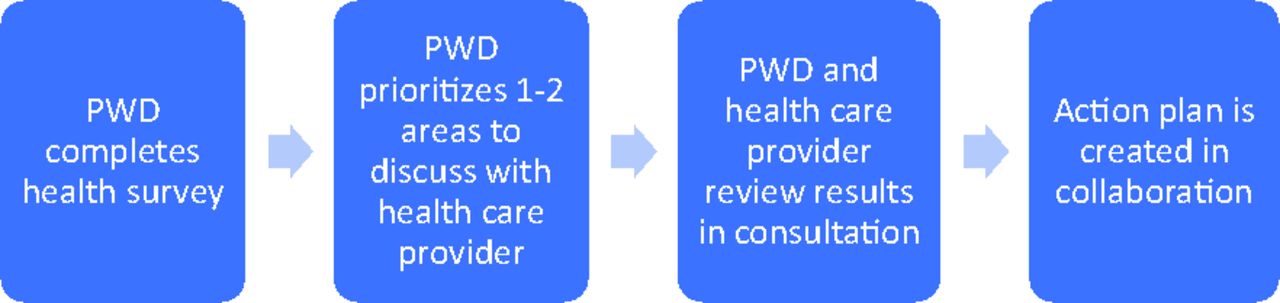
The CTH program guides patients and health care providers through multiple steps: (1) the PWD completes an electronic health survey that assesses 15 areas of self-management and contextual circumstances that may impact self-management (Figure 1), and identifies possible self-management problems; (2) based on the reviewed survey results, the PWD prioritizes 1 to 2 areas they want to discuss with their health care provider; (3) the health care provider review the results with the PWD; and (4) in collaboration, the PWD and health care provider selects a goal from a list of the identified self-management problems or a custom goal and create a detailed action plan (Figure 2). The electronic action plan is structured with written prompts and free text space to guide the provider and PWD through steps of action planning, including goal selection, brainstorming actions (what the PWD will do), selecting and creating a detailed plan for 1 action (when, how often, where), barriers to acting on the plan, and confidence in carrying out the plan.

Self-management Problems Used as Goals in Action Plans.

Outline of the Connection to Health Steps. Abbreviation: PWD; person with diabetes.
As a part of the study design, practices selected a subset of 2 to 5 health care providers who would participate in a 6-hour training program that included an introduction to SMS and a group-based, live tutorial on how to use the CTH system. Providers in EE-CTH received the same training as well as additional training in engagement and relationship-building skills. The protocol was approved by the University of California, San Francisco Institutional Review Board (15-17033).
Measures
Health Survey
The patient health survey captures key patient demographic factors, including age, sex, educational level, race and language (English or Spanish), and 15 areas of behavioral self-management or life context. Given the focus on factors from an individual's life context that may influence their action plan quality, the following areas were selected. Health literacy was measured by the single screener item “How confident are you filling out medical forms by yourself?” on a 5-point scale ranging from “not at all confident” to “extremely confident.”30
Mental health measures included depression symptoms,31,32 health distress,33,34 and general life stress.35 Depression symptoms were assessed using the Patient Health Questionnaire-8 (PHQ-8; omitting the suicidal ideation item) with a score range of 0 to 24 (elevated symptoms noted by scores of 10 or greater).31,32 Health-related distress was measured using a modified version of the Diabetes Distress Scale 2-item screen (DDS-2): “How much of a problem have the following been for you over the past month?” (1)“ Feeling overwhelmed by my health problems” and (2) “Feeling that I was failing to do what I should be doing to manage my health problem” on a 5-point scale ranging from “not a problem” (1) to “a very serious problem” (5) (elevated symptoms noted by mean scores of 2 or greater).33,34 General life stress was assessed with the single item: “In the past week, have you been under a lot of stress due to a major change or event or from a stressful situation (for example, family, work, or financial problems)?” using a yes/no response option.35
Finally, social risks were measured by 6 items (yes/no) developed in previous work using the following question: “Are you experiencing any of the following?” (1) “Running out of food before having enough money or food stamps to buy more,” (2) “Problems paying bills, like electric, gas, water, or phone bills,” (3) “Not having enough money to pay for bus fare or access to reliable transportation to medical appointments,” (4) “Unstable housing including eviction, foreclosure, homelessness or staying with friends/family,” (5) “Have you been hit, slapped, kicked, or physically hurt by someone in the past year?”, and 6) “Do you feel safe where you live?”36⇓–38 Additional behavioral measures of the health survey included: diet,39⇓–41 physical activity,42 medication adherence,43⇓–45 tobacco use,46,47 and alcohol consumption.48,49 These were included as action plan goals areas but not as predictors of action plan quality.
Confidence in carrying out the action plan was measured on a scale of 0 to 10 after action plan completion, with low scores indicating low confidence in carrying out the plan and high scores indicating high confidence.13,14 In the current study, efforts were made to assure that each patient had a minimum level of confidence in their plan before it was completed. Providers were encouraged, but not required, to continue working on each action plan with patients until a confidence level of ≥ 8 was reached.
Action Plan Quality
Text from action plans was electronically captured by the CTH/EECTH system and coded by members of the research team using an adapted version of the previously validated Goal-Setting Evaluation Tool for Diabetes (GET-D). GET-D is a coding system that enables reliable and valid ratings of the quality of written goals and action plans.50 To characterize inter-rater reliability (IRR), 20% of action plans were dual coded to reach an IRR of > 80%. See Table 2 for the 8 coding elements and scoring. One aspect of the GET-D, whether the action plan is feasible for the patient to carry out or not,50 was omitted because of its potential subjectivity.
Data Analysis
Descriptive statistics were computed to document score distributions. Tests of association between the dimensions of action plan quality and patient and practice level variables were initially examined in unadjusted analyses including Pearson's and Spearman's correlations for continuous and ordinal variables, respectively. To adjust for clustering by clinic and intervention arm, the same associations were then calculated using Generalized Linear Mixed Models (GLMM) with a random effect for clinic and intervention arm. Data were analyzed using SPSS v.26 software (IBM, Armonk, NY).
Results
Across the 12 clinical sites, 725 patients completed the health survey and made an action plan in consultation with a health care provider (n = 382 for CTH and n = 343 for EE-CTH). Patient participants were on average 55.6 (±12.0) years of age, 59.7% were female and 41.0% had not completed high school. The majority identified themselves as Latinx (70.5%); 56.4% completed the assessment in Spanish with the remaining in English. The health survey indicated elevated symptoms of depression (PHQ score of ≥ 10) in 15.8% of the patients and 46.3% reported having ≥ 1 social risk factor. Patient characteristics are presented in Table 1 with group differences noted where the differences reached statistical significance.
Patient Characteristics
Thirty-seven health care providers across the 12 clinical sites delivered the action planning protocol as part of CTH or EECTH. Providers were a mix of health educators (24.3%), patient navigators (18.9%), medical assistants (18.9%), volunteers (16.2%), nurses (10.8%), dieticians (8.1%), and physicians (2.7%). There was no difference in action plan quality by provider role, except for relatively lower quality action planning by patient navigators compared with all others (all comparisons P < .005).
Quality of Action Plans in Primary Diabetes Care
Overall, the quality of action plans assessed by the GET-D across clinics was moderately-high with a mean score ± SD of 14.62±3.87 on a 0 to 20 quality scale. While all action plans identified a diabetes management goal, the greatest variability occurred around action plan specificity and plan details (eg, frequency, locations; Table 2). Most action plans focused on different aspects of diet (41.9%) or physical activity (30.2%); a smaller number of patients made action plans focusing on weight (8.0%), taking medications (6.1%), and general life stress (4.8%) (Figure 3). Mean action plan quality across the 12 clinics ranged from 12.39 ± 3.71 to 16.97 ± 2.84. Statistically, significantly higher quality plans were created in clinics using the CTH program with a mean quality of 15.10 ± 3.73 compared with 14.10±3.96 in clinics using the EE-CTH program (t(723)=3.49, P = .001). Given the statistically significant between-group difference, we adjusted all GLMMs to control for intervention conditions (CTH and EE-CTH).
Goalsetting Evaluation Tool for Diabetes (GET-D)50

Most Prevalently Selected Self-Management Areas; (n = 725).
Patient Characteristics Associated with Action Plan Quality
Lower patient health literacy was significantly associated with lower action plan quality (P = .007): individuals who endorsed having the most difficulty around health literacy had a mean score and SD of 13.62± 3.85 compared with those who expressed no difficulty with a mean score of 14.63 ± 3.88. The presence of social risks was also related to action plan quality (P = .021); individuals who reported having at least 1 social risk had a mean (S.D.) quality score of 14.37 ± 3.94 versus 14.84 ± 3.81 for those with no social risks. Among the individual social risks, only physical abuse, endorsed by 3.3% of the sample, reached statistical significance (Table 3). Other life contextual variables examined, including depression symptoms, general life stress, and health-distress were all unrelated to action plan quality. Patient demographic factors (age, sex, language, education level) also were unrelated to action plan quality, except for race. Individuals who identified as multi-racial or Native Hawaiian/Pacific Islander received lower action plan quality scores compared with individuals identifying as Latinx (P = .045 and 0.057 respectively), though the sample size for both groups was small (n = 36 and 12 respectively). Furthermore, there was no association between action plan quality and the self-management area targeted for change, for example, diet, physical activity, or stress (rs = −0.002, P = .954). Nor was there a pattern of significant interactions between the intervention arm (CTH vs EE-CTH) and patient characteristics or life contextual variables.
Associations Between Action Plan Quality and Patient Characteristics. Analyzed Using Generalized Linear Mixed Models With Random Effect for Clinic, Adjusting for Intervention Arm
Action Plan Quality and Patient-Reported Confidence in Carrying Out the Plan
On average, patients had high confidence in carrying out their plans with a mean confidence level of 8.56 ±1.58 on a scale of 0 to 10. The patient's confidence in carrying out their action plans was positively related to the quality of the action plan (n = 725, β = 0.050, standard error [SE] = 0.018, 95% CI, 0.016–0.084, P = .004). Confidence level was also related to race: identifying as non-Latinx white was associated with relatively lower confidence of 8.28 ±1.50 in carrying out the plan (β = −0.310, 95% CI, 0.599–0.020; P = .036) compared with Latinx with a mean confidence of 8.59 ± 1.62. Confidence level was not significantly associated with any other demographic or patient-reported index.
Discussion
While action planning is a cornerstone of primary care frameworks including the PCMH and CCM2⇓⇓⇓–6 and associated with improved diabetes outcomes,15⇓⇓–18 little work to date has examined either objective ratings of action plans in primary care or correlates of action plan quality to inform efforts in improving our quality of care and driving change. This study examined the assessed quality of action plans using the GET-D in the context of a pragmatic trial with adults with T2DM in CHC settings using an electronic program to support SMS. Findings indicate that, overall, the action plans created were of moderate to high quality, and that select patient life contextual factors are linked with quality. Patient health literacy is linked with higher quality action plans. This suggests that individuals with lower health literacy may need additional support from the health care setting to create viable action plans. Multiple studies have focused on the need to address low health literacy in primary care. A study from 2011 examined different approaches and created a toolkit for primary care practitioners.51 Likewise, individuals who endorsed social risks had on average action plans of lower quality. These individuals may be navigating several competing life stressors or experiencing challenges prioritizing disease management changes within this context. Under a recent National Academy of Medicine report, we suggest that collaborative action planning may need to be tailored or adjusted to take an individual's social risks and context into account.23,52
Even though efforts were made in the present study to assure that each patient had a minimum level of confidence in their plan before it was completed, there was still considerable variation in patient-reported confidence. Higher confidence is positively associated with the quality of the action plan. Previous literature has focused on the importance of perceived confidence as a potential indicator of future behavior change.14,19 Future longitudinal work should examine whether higher confidence leads to greater success in goal achievement.
We find that the quality of action plans is not associated with age, sex, language (English or Spanish), or educational level. This suggests that this type of goal setting and action planning can be implemented across diverse patient groups with no apparent difference in the quality of the implementation. There is, however, a significant association between quality and race, in which individuals identifying as Native Hawaiian/Pacific Islander or multi-racial have relatively lower action plan quality scores. Given the mixed nature of the multi-racial sample and the relatively small sample size of each, we are unable to examine this finding further based on a specific racial group. Furthermore, there is no relationship between action plan quality and symptoms of depression, health distress, or general life stress, suggesting that individuals experiencing these characteristics can engage in creating moderate to high-quality action plans despite their distress. In line with previous work, we note that most action plans focus on diet, weight loss, or physical activity1. However, no association between the type of action plan target and quality of action plan is seen; nor is there a systematic association between action plan quality and provider role (eg, medical assistant). These findings suggest that high-quality action plans can be collaboratively developed between PWD and a variety of different types of providers and across a variety of action plan targets or goals.
A statistically significant, modestly higher level of action plan quality is seen in CTH compared with EE-CTH, although this difference is not related to any subsequent study findings. As clinics had the freedom to select the patients they wished to work with, the statistically significant group differences are not unexpected. The differences in action plan quality between CTH and EECTH may have in part been due to the group differences in relevant patient characteristics, in which the patients selected for EECTH had on average lower health literacy and more patients identified as multi-racial. In addition, the GET-D rating system itself may have played a role: the ratings tend to emphasize specific behavior change actions (time, location, duration, etc), with much less emphasis on issues of engagement and motivational barriers. These findings highlight the potential need for broadening the concept of action plan quality to include engagement, motivation, and confidence in carrying out the plan.
Study limitations include the restriction to CHC's serving a multi-ethnic English or Spanish speaking safety net population in 1 geographic area, which may limit generalizability to other primary care settings. It also was not possible to link action plan quality with specific provider characteristics, nor additional characteristics of the clinic. This would be valuable to explore in future studies. Finally, further work is needed to examine the associations between action plan quality and subsequent clinical outcomes, which will be the subject of a future report.
Conclusion
Results of this study provide a window into assessing the quality of action planning for diabetes in primary care and point to patient characteristics associated with quality that can guide future SMS efforts tailored to individual patient contexts. Overall, both the CTH and EE-CTH programs enabled health care providers to develop moderate to high-quality action plans with their patients with type 2 diabetes. Higher health literacy, having no social risks, and identifying as multi-racial are significantly related to higher quality action plans. This finding suggests a potential benefit to tailoring the action planning process according to health literacy, social risks, and racial context. Higher quality action plans also are associated with greater patient confidence in carrying out the action plan, underlining the potential value of a comprehensive patient-centered approach to action planning. Further research is needed to establish the relationship between action plan quality and diabetes management change as well as longer-term clinical outcomes.
Acknowledgments
We wish to acknowledge all participating clinical sites - including healthcare providers and leaders as well as all participating patients. We want to acknowledge the San Francisco Bay Area Collaborative Research Network (SF Bay CRN, sfbaycrn.org) for support and assistance with clinical site recruitment and engagement in the study. This work was supported by a grant from the Lundbeck Foundation to the Innovation Centre Denmark, Silicon Valley to fund the Danish American Research Exchange for Pernille Kjaer at the Department of Family Medicine at the University of California, San Francisco.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: This research was funded by NIH Grant DK108039. Lundbeck Foundation grant.
To see this article online, please go to: http://jabfm.org/content/34/3/608.full.
- Received for publication June 10, 2020.
- Revision received November 20, 2020.
- Accepted for publication November 22, 2020.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Methods
- Measures
- Action Plan Quality
- Data Analysis
- Results
- Quality of Action Plans in Primary Diabetes Care
- Patient Characteristics Associated with Action Plan Quality
- Action Plan Quality and Patient-Reported Confidence in Carrying Out the Plan
- Discussion
- Conclusion
- Acknowledgments
- Notes
- References
- Figures & Data
- References
- Info & Metrics