
Abstract
Purpose: Meaning in work has been identified as an important factor promoting physician resilience against burnout. However, research has only minimally explored meaningful patient-physician relationships in relation to physician burnout, and has largely focused on patient perspectives. To address this knowledge gap, this study explored the elements of relationships with patients that physicians find meaningful, as well as physicians' perceptions of how those relationships influence experiences of burnout.
Methods: In this qualitative study, 20 family medicine physicians recruited via convenience and snowball sampling participated in semistructured interviews. The research team then engaged in an iterative process of thematic analysis.
Results: 5 main themes emerged in participants' descriptions of meaningful relationships with their patients: Patient-centered care, continuity, effective care, trust, and purpose and mission. Participants described meaningful relationships as situated within a professional mission to connect with patients and make a difference in their lives. Meaning in these relationships centered around a trusting therapeutic relationship formed through continuity, person-centered care, and effective care. Participants strongly felt that meaningful relationships with patients are protective against burnout.
Conclusions: Though many burnout interventions have targeted change at the individual (physician) level, a growing amount of evidence points to the need for change at the health system level. The findings of this study suggest that system-level interventions aimed at enhancing and prioritizing physicians' experiences of continuity and connection with their patients may be particularly impactful in efforts to reduce and prevent burnout.
- Delivery of Health Care
- Family Medicine
- Patient-Centered Care
- Physicians
- Primary Health Care
- Qualitative Research
- Workforce
Estimates indicate over half of all US physicians experience burnout, a syndrome characterized by emotional exhaustion, depersonalization, and feeling ineffective.1 Compared with the general working population, physicians are at markedly increased risk of burnout and dissatisfaction with work-life balance.1 This risk is even greater for primary care physicians, who experience higher levels of burnout than other specialties,2 with administrative burdens, increasing productivity expectations, and feeling undervalued as major contributors.3⇓⇓⇓–7 Family medicine, in particular, frequently ranks in the top specialties experiencing the most burnout.8,9
A sense of meaning in work has been identified as a central protective factor against burnout.10⇓–12 For many primary care physicians, continuity of care and the development of long-term, caring relationships with patients is a major motivating factor in their career choice.13 However, changes in the health care system requiring physicians to see more patients in less time have become a barrier in the development and maintenance of these meaningful relationships.14 Thus, physicians are facing increased work demands, but with fewer of the meaningful experiences that were among the reasons they originally chose a career in primary care.15
Though meaningful work has been identified as a factor promoting physician resilience against burnout,10,16⇓–18 current research has only minimally explored meaningful patient-physician relationships in relation to burnout. Current literature lacks a clear definition of a “meaningful” patient-physician relationship. In addition, the patient-physician relationship is most frequently studied from the patient perspective, with physician perspectives of this important aspect of their work largely absent in the literature.19 Understanding how these relationships protect physicians against burnout can support future research on burnout prevention and inform both interventions and health care reform. The current study aimed to address the following 2 research questions: (1) How do family physicians describe meaningful relationships with patients?, and (2) How do family physicians perceive meaningful relationships with patients as influencing their experiences of burnout?
Methods
We used a descriptive phenomenological approach to describe family physicians' experiences of meaning in their relationships with patients and explore their perceptions of how these relationships influence their experiences of burnout. The University of Texas Southwestern Medical Center institutional review board approved this study.
Sample and Data Collection
Family physicians were recruited via convenience and snowball sampling through listservs affiliated with primary care professional organizations and the research team's institution.20 Participants were required to be family physicians actively practicing at the time of recruitment. All participants completed a demographic questionnaire and semistructured interview (see interview guide in Table 1).
Interview Guide
Three members of the research team conducted interviews and were trained in qualitative interviewing techniques to ensure uniformity of process and depth of data. All interviews were audio-recorded, and participants were given the option of conducting the interview via phone or video, or in-person at a location of their choice. Because burnout can be a vulnerable topic, participants were offered mental health resources if desired.
Analysis
Two members of the research team (ARH, a relationship researcher, and PC, a medical student going into family medicine) led this qualitative analysis, engaging in an iterative process of thematic analysis.21 To assess for saturation of themes, data analysis began before the end of recruitment, which was concluded once no new themes were emerging.22 This analysis team began by coding the first 7 transcripts independently, then creating a codebook and initial coding structure based on emergent themes. To create the initial coding structure, all individual codes were reviewed collectively, and organized into midlevel categories. Each coder applied the initial coding structure, independently, to an additional 3 transcripts to review the coding structure's fit to the data. After adjustments to the coding structure, this process was repeated with another 3 transcripts, at which point the analysis team confirmed fit to the data. Within this coding structure, the analysis team then identified connections and relationships between the themes.
To ensure rigor and trustworthiness of the analysis and interpretation through additional triangulation,23 the remainder of the research team (3 family physicians and 1 relationship researcher) reviewed the coding structure and provided feedback regarding quality of the analysis and clarity of the coding structure. This feedback was incorporated into the final coding structure. The research team additionally engaged in a process of reflexivity regarding any influence of educational training and prior experiences on the data analysis. The research team was intentionally formed with members of different academic backgrounds and career stages, creating a diverse range of perspectives to enhance rigor for a rich and trustworthy analysis.
Results
Twenty-eight family physicians responded to the study's recruitment, and of these, 20 completed the interview. Interviews were conducted between June 2019 and March 2020. Participant demographics and a summary of emergent themes and subthemes are presented in Tables 2 and 3, respectively.
Participant Demographics (n = 20)
Summary of Themes and Sub-Themes
Research Question 1: Elements of Meaningful Patient-Physician Relationships
Participants described 4 main elements of meaningful patient-physician relationships, situated within an overarching sense of purpose and mission to connect with patients and make a difference in their lives (see Figure 1). Three of the elements emerged as a cyclic relationship, with person-centered care leading to a sense that the care offered was effective, and therefore building continuity, further enhancing person-centeredness. In descriptions of each of these, the participants repeatedly identified trust as a common thread that both grows from these elements and enhances them over time.
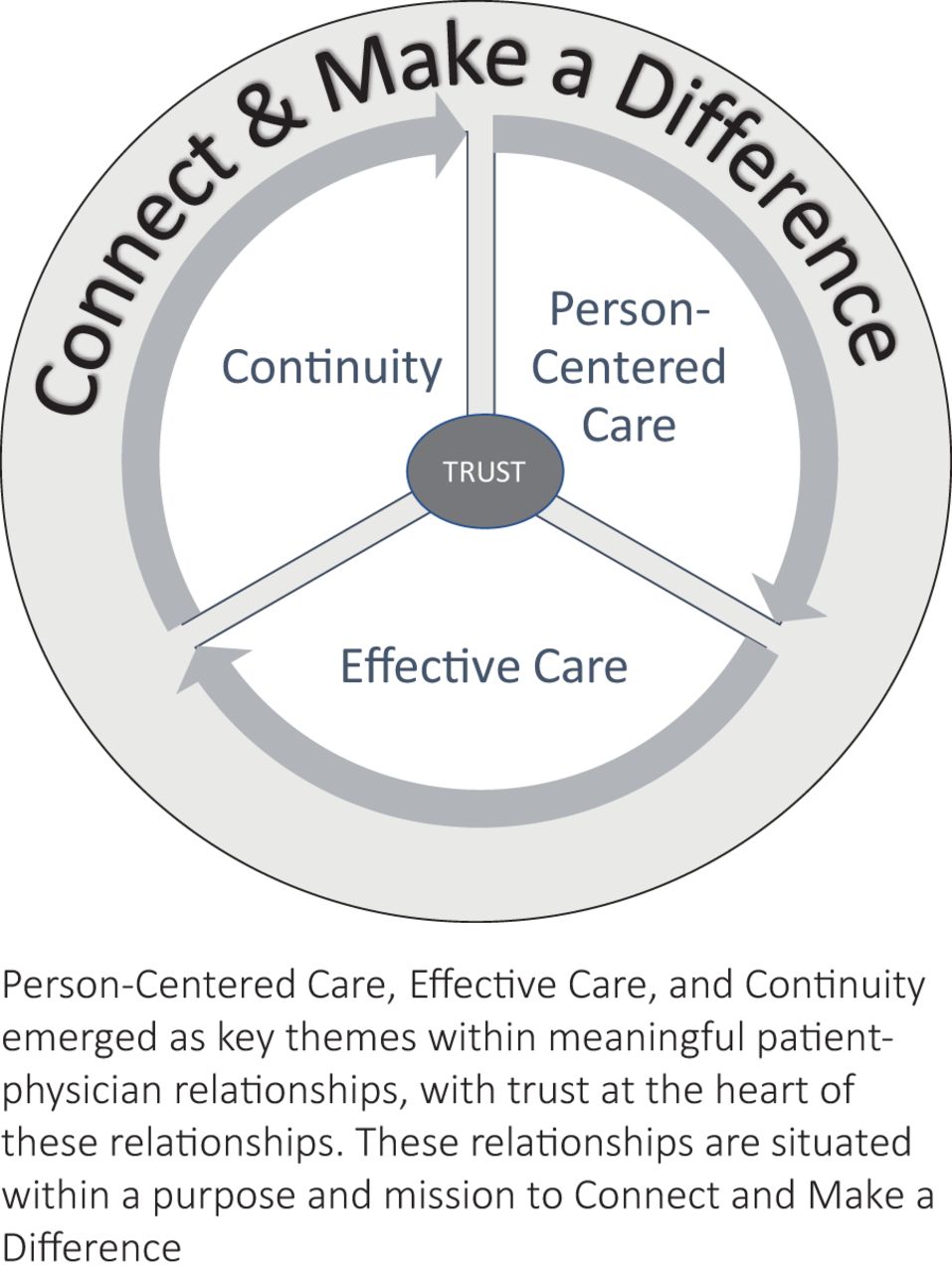
Components of meaningful relationships with patients.
Person-Centered Care
Many participants found meaning in “treating [patients] as people,” beyond “just treating their symptoms.” It was important to them to have an in-depth knowledge of their patients, tailor care to each patient, and develop a partnership in that care:
Shared decision making is the thing that I value in the relationship. Although the physician brings the knowledge, spends so much time training and being up to date, you have that knowledge and the patient has the other knowledge that is needed to put those two pieces together.
Knowing patients as human beings and partnering with them in their health care was a significant source of meaning, and contributed to a sense of connection and trust:
Getting to know them beyond why they're here…Learning about their families…It helps me gear my visits to better serve them. So with every visit for me, it's who are you and how did you get to where you are? And once I'm able to get that, I feel like we break that ice and you trust me to take care of everything else.
Effective Care
While clinical effectiveness is often measured by objective metrics related to productivity and health outcomes, the participants in this study expressed the importance of a different kind of effectiveness. From their perspectives, the connection and trust formed through knowing their patients as humans facilitated problem solving and patient engagement in health behaviors and created space for patients to be open and vulnerable, elements they felt increased their effectiveness as physicians. This contributed to meaning in those relationships and in their work more broadly:
So there's a patient with a health concern who offers sensitive information, because of that trust. And then we're able to do something about it with that information that ends up helping the patient. That, for me, is the most meaningful.
Overall, the participants felt satisfaction and purpose in the quality of care they provided, a high quality enhanced by a person-centered approach:
To know that you're actually giving them solid care, solid human care, is something that is meaningful to me even on my worst days…If I'm able to help [patients] out, that's very meaningful to me, to know that I'm providing that care that I'm supposed to be providing.
Continuity
Continuity was an essential component in their descriptions of meaningful relationships with patients. The opportunity to work with patients over long periods of time and, in some cases, across both outpatient and inpatient settings was described as contributing to trust, connection, and a deeper knowledge of patients' lives and medical needs:
It's the extent of those relationships over time, gives me a sense that we've developed a real depth to our therapeutic relationship. I have known them through a number of different circumstances and situations and illnesses, and they have also seen me develop professionally…Those relationships are rich because they've been going on for a long time.
Continuity was also described as helping “encounters become more meaningful over time, because there's an established relationship, an established rapport, and there's trust.” For these participants, length of the relationship often correlated with the depth of meaning felt in those patient encounters, as a result of the connection that has grown over time. The development of that trusting relationship over time in turn enhanced the person-centered approach:
Continuity helps you make sure that you're always on the same page as far as priorities and values and what you want to accomplish with them and what they want to accomplish with you.
Trust
A trusting therapeutic relationship was at the heart of the participants' descriptions of meaningful relationships with their patients, with 1 participant saying, “If I had to pick just one word, that would be trust.” For these participants, trust helps patients share vulnerable information, and is built over time as patients experience their physician as compassionate, nonjudgmental, competent, and responsive. Trust was a common thread present throughout each other theme. A patient-centered approach, delivery of effective care, and continuity in the patient-physician relationship created fertile ground for trust to grow, but that trust further enhanced each of those elements.
Purpose and Mission
Together, these elements of meaningful patient-physician relationships contributed to a sense of purpose in the participants' work. While describing their meaningful relationships with patients, the participants identified these relationships as fulfilling purpose in two ways: the ability to make a difference in their patients' lives and forming connection with their patients. One participant described this combination succinctly: “I love taking care of them and love being a part of their lives.” Making a difference and creating strong connections were described as essential factors in participants' choices to become a physician, and as key elements of their missions as family physicians, specifically. Speaking of connection, one participant stated:
Most of us in primary care went into this field [because] we love people. We love interacting with people. We love building that relationship with people.
And ultimately, the strongest desire is to care for people who need help: “When we're able to do something that ends up helping the patient in a particular way, that, for me, is the most meaningful.” As one participant stated, meaningful relationships with patients “remind you the reason why you are doing it.”
Research Question 2: Impact of Meaningful Patient-Physician Relationships on Burnout
All 20 participants felt that meaningful relationships with patients provide a protective benefit, though 7 participants described ways these relationships can also inadvertently contribute to burnout.
Protective against Burnout
Descriptions of the protective nature of meaningful patient relationships highlighted 2 main factors contributing to this protective benefit: fulfillment of a sense of purpose and significance, and the ability of continuity in the patient-physician relationship to ease workload. Speaking of purpose and significance, one participant described the satisfaction and joy she experiences in helping her patients:
That meaningful relationship is a protective factor against burnout. You get a sense of satisfaction in what you do. You're helping someone, but also helping yourself in some way because joy is contagious…That's the reason we do this. Because we want to care for people.
Through building meaningful relationships with patients, many participants identified continuity as an important result of those connections, bringing additional protective benefits against burnout:
Having those connections makes it easier…because I already know the person's history and situation, and it does make it easier to dig down into what they want from the visit and what the plan should be and what their diagnosis is.
Contributing to Burnout
For the 7 participants who described meaningful patient relationships as both protective and potentially contributing to burnout, the contributing factors arose because of the connection and care in those relationships. Specifically, these descriptions fell into 2 subthemes: striving for excellence in a broken system, and seeing beloved patients suffer. The participants described the deep frustration in feeling their hands are tied in their efforts to provide high quality care. This includes the “financial disincentive to spend more time with [patients]” and funding and access limitations, as exemplified by this participant:
Unfortunately, we are trying to adjust a system issue with an individualized treatment, getting people to do yoga, exercise, and all kinds of good things, which will probably help with the individual problem. But it's not going to solve, for example, my patient not getting his medications. It's not going to resolve an issue with my patient not getting his MRA approved. And that is what frustrates you as a physician.
Because of the participants' connection with their patients, several described the pain of seeing their patients suffer, speaking of suffering both in terms of the limitations of the health care system and the normal toll illness takes on those experiencing it:
When [patients] are going through those tough times and even when they pass away, it wears on me…. If I didn't care about my patient, and didn't have the relationship, it wouldn't bother me. It would not create burnout. It's just part of the job.
While reflecting on the ways meaningful relationships prevent or reduce experiences of burnout, the participants lamented the many “nonpatient care” barriers in their work that contribute to burnout by impeding their ability to engage further in those meaningful connections that create a sense of purpose and significance in their work. These included long work hours and work being taken home because there is no time between patients, a loss of autonomy in practice management decisions, time-consuming administrative tasks, and the pressure to see more patients, with emphasis on volume rather than quality of care. As a result of these burnout-inducing factors, the participants described exhaustion, depression, lack of satisfaction in their work, taking longer to complete tasks, disappointment in their work performance, isolation from loved ones, and even consideration of leaving medicine altogether. Their descriptions highlight meaningful relationships with patients as a key factor in efforts to understand and prevent physician burnout.
Discussion
Four main themes emerged in the participants' descriptions of meaningful patient-physician relationships: person-centered care, effective care, continuity, and trust. These themes were situated within a context of mission and purpose in connecting with patients and making a difference in their lives. These findings build on a prior study's investigation of physicians' perspectives on meaning in medical practice more broadly that highlighted 3 major themes: a fundamental change in the physician's perspective, connection with patients, and a difference made in a patient's life.12 Nearly 20 years later, the present study further emphasizes connection and making a difference as key elements in physicians' work and extends this exploration specifically to the patient-physician relationship. This is the first study, to the investigators' knowledge, to form a definition of “meaning” in patient-physician relationships from the physician's perspective.
All participants in this study viewed meaningful patient-physician relationships as protective against burnout. This finding aligns with previous research connecting meaning in work to reduced likelihood of experiencing physician burnout,10⇓–12,18 and extends this line of research by exploring this protective factor as it relates to the practice of family medicine specifically. With a clear model of meaning in family physicians' relationships with their patients (Figure 1) and data to support it, we can improve our approach to physician burnout through enhancement of these factors contributing to meaning, while addressing factors that inhibit the development of meaningful patient-physician relationships.
Participants' descriptions of ways in which meaningful relationships can contribute to burnout add important nuance to discussions regarding burnout prevention and intervention. The emergent themes in these descriptions (striving for excellence in a broken system and seeing beloved patients suffer) both stem from an interruption in purpose, a key element in meaningful relationships with patients. These participants described an inability to help, feeling in many circumstances that they have the training to make a difference in their patients' lives, but their hands are tied by the health care system.
Beyond the context of the patient-physician relationship, participants also described more generally that not having enough time with patients and experiencing the current health care system as limiting their ability to provide high quality care to all patients are significant contributors to burnout. Both of these relate directly to the overarching theme within meaningful patient-physician relationships that emerged in this study: A sense of purpose and mission in connecting with patients and making a difference in their lives. Thus, burnout prevention cannot be a simple call to ‘go forth and connect with your patients.’ Addressing the barriers that inhibit physicians' abilities to cultivate the elements of meaning in relationships with patients is critical to successful burnout prevention.
These findings align with a recent study connecting burnout to professional dissonance, which many primary care physicians experience as they work in health systems that hold values that differ from their values as clinicians.25 Aligning these values and enabling physicians to devote more time to the most meaningful elements of their practice have been identified as 2 effective strategies for addressing the physician burnout crisis.4 Data from this study contribute to the growing evidence base indicating the need for burnout intervention strategies to target barriers to physician wellness at the health system level, particularly in regard to enhancing elements of practice that physicians find most meaningful, rather than relying primarily on individual-level interventions (eg, “self-care,” meditation).6,27⇓–29 Though interventions at the individual level are important and should not be abandoned, in many cases these can simply be a bandage on a wound requiring a higher level of care.
Truly system-level intervention efforts will likely benefit from using the 3-World View health care framework described by C. J. Peek,30 intervening across the clinical, operational, and financial spheres. Peek asserts that problems arise when these 3 contexts become unbalanced. Physician burnout may represent 1 symptom of an imbalance in which the clinical and operational worlds have been overshadowed by financial priorities. A recent systematic review of predictors of physician burnout identified many modifiable factors across these 3 worlds that interventions can target at a system-level: lack of values alignment between physicians, administration, and leadership; low satisfaction with resources needed to care for complex patients; decreased practice autonomy; low emphasis on quality of care; low organizational trust and workplace cohesiveness; greater time pressure; low promotion of work-life balance; and working extended hours during evenings/weekends.31 Though by no means simple, an increased focus on cultivating medical practices that fulfill family physicians' missions to connect with their patients and make a difference in their lives, coupled with purposeful collaboration across the 3 worlds, may prove more effective in moving the needle on physician burnout.
Limitations and Future Directions
The participants in this study were exclusively from the field of family medicine. It is possible that these findings may vary across specialties, particularly those outside primary care in which there is less emphasis on continuity of care and patient-physician relationships. Additional research involving other disciplines is needed to determine if there are themes of meaningful patient-physician relationships common to all physicians, as well as investigate important differences across specialties. If identified, these elements can guide future health care policy at both cross-discipline and discipline-specific levels for more effective burnout intervention. As an additional limitation to generalizability, this study utilized snowball sampling, and physicians experiencing meaningful relationships as protective against burnout may have been more likely to respond to study recruitment and elect to participate.
This study did not separately examine the contribution of practice context. It is likely that practice structure (eg, private group practice, direct primary care) may influence physicians' experiences of meaningful patient-physician relationships and burnout. While this study had a diverse sample in regard to practice setting and stage of career, future studies investigating differences among these demographics are needed. Lastly, studies testing the effectiveness and feasibility of system-level burnout interventions are an important next step, with voices represented from all levels of health care practice.
Conclusion
This study outlines the key elements of family physicians' meaningful relationships with patients, and how these relationships influence experiences of burnout. For these family physicians, meaningful relationships exist within an overarching mission to connect with patients and make a difference in their lives, and encompass person-centered connections with patients, care that is effective in making a difference in patients' lives, continuity of these relationships, and patients' trust in their physician's efforts and expertise. Each participant described meaningful relationships with patients as protective against burnout, but these meaningful relationships can also contribute to burnout when physicians' missions to connect and make a difference are interrupted, through witnessing suffering in patients with whom they have a strong connection and feeling unable to help patients due to limitations of the health care system. This study contributes to the growing literature base indicating the need for system-level burnout interventions that aim to enhance the meaningful aspects of family physicians' work and bring greater alignment and collaboration across the 3 worlds of health care practice.
Notes
This article was externally peer reviewed.
Funding: This study was unfunded.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/4/716.full.
- Received for publication November 4, 2021.
- Revision received February 7, 2022.
- Revision received March 18, 2022.
- Revision received April 8, 2022.
- Accepted for publication April 25, 2022.




{kind=link}