
Abstract
Introduction: Rates of infant vitamin D supplementation fall short of guideline recommendations. We explored this discrepancy from the clinician perspective as they advise and affect this important intervention to prevent rickets. We compared infant and high-dose maternal vitamin D supplementation prescribing attitudes and practices between infant-only clinicians (IC) and clinicians who care for mothers and infants (MIC).
Methods: We surveyed clinicians in departments of family medicine, obstetrics/gynecology, primary care pediatrics, neonatology, newborn nursery, and members of vitamin D and rickets working groups and a social media group for lactation medicine providers about their perspectives and practices regarding vitamin D supplementation.
Results: 360 clinician survey responses were analyzed. In current practice, IC were more likely than MIC to recommend vitamin D supplementation to exclusively (P < .001) and partially breastfed infants (P = .005). MIC were more likely than IC to discuss infant and high-dose maternal supplementation options and let the parents/caregivers choose (34.7%, 22.0%, P = .009). If supplementing the mother with high-dose vitamin D or the infant directly each provided adequate vitamin D in the infant, MIC were more likely than IC to think that supplementation of the mother would be preferred by parents/caregivers (63.0%, 45.2%, P = .003), improve adherence (66.5%, 49.4%, P = .006), and promote breastfeeding (54.7%, 36.5%, P = .001); they were also more likely to recommend supplementation of the mother (17.7%, 8.9%, P = .04).
Conclusions: MIC are more likely than IC to embrace high-dose maternal vitamin D supplementation to provide adequate vitamin D for infants. This highlights an opportunity for further education of clinicians about this option.
Introduction
Vitamin D is necessary in infants to prevent rickets, reduce the risk of life-threatening complications of hypocalcemia,1,2 strengthen the immune system,3,4 and support prevention of cancer, diabetes, and other chronic diseases.5⇓–7 Although the prevalence of rickets is considerably lower than it was a century ago, the rates of nutritional rickets are climbing, with an incidence of 24 per 100,000 children under 3 years in the decade beginning in 2000 in Olmsted County, Minnesota.8 Breast milk from unsupplemented mothers does not provide enough vitamin D to infants,9⇓–11 and very young infants do not consume enough fortified formula to ensure sufficient levels. Therefore, vitamin D supplementation is recommended for infants in the US and globally.12,13 Infants can receive supplementation directly with oral vitamin D drops or indirectly through breast milk from women who receive daily (4000 to 6400 IU/day [100 to 160 mcg/day]) or monthly (120,000 to 150,000 IU/month [3000 to 3750 mcg/month]) high-dose vitamin D.11,14⇓⇓–17
Due to continued cases of nutritional rickets and inadequate sunlight exposure, the American Academy of Pediatrics (AAP) revised its guideline on infant vitamin D supplementation in 2008. The guideline recommended increasing supplementation of vitamin D from 200 to 400 IU per day starting in the first few days of life for all infants less than 1 year of age who are exclusively or partially breastfed and nonbreastfed infants who consume less than 1000 mL of formula per day.9 The Institute of Medicine18 formally supported this guideline in 2011 as did an international nutritional rickets consensus group in 2016.19 Despite these changes, between 2009 and 2016, only 27% of US infants received the recommended amount of vitamin D, and there was no significant improvement in the proportion of infants who met the guideline.20,21
Given that rates of infant vitamin D supplementation fall short of guideline recommendations, we explored this problem from the perspective of the clinician as they advise and affect this important intervention to prevent nutritional rickets. Our primary objective was to compare infant and maternal vitamin D supplementation prescribing attitudes and practices between infant-only clinicians (IC)—clinicians in primary care pediatrics, neonatology, and those who work primarily in the newborn nursery—and clinicians who care for mothers and infants (MIC)—family medicine and obstetrics/gynecology clinicians. We hypothesized that MIC are more likely than IC to recommend high-dose maternal supplementation. Second, we postulated that both groups follow infant vitamin D supplementation guidelines at similar rates.
Methods
Design
We performed a voluntary, cross-sectional survey study using the online survey platform “Qualtrics” (Qualtrics software, Provo, UT, Version April 2021). The survey included 33 questions about attitudes and practices around vitamin D supplementation of infants and mothers, perceived parent/caregiver adherence to supplementation recommendations, experience with children with nutritional rickets and vitamin D toxicity, and demographic questions (Online Appendix). The survey was not formally validated, but a similar survey study was previously published by members of the research group22 and served as a framework for the current survey. The platform’s usability and technical functioning were tested before survey distribution. The study was reviewed and approved as exempt by Mayo Clinic and Nemours Institutional Review Boards.
Sample
The survey was sent by e-mail to 2325 clinicians at Mayo Clinic and Mayo Clinic Health System (Minnesota, Wisconsin, Florida, Arizona), as well as Mayo Clinic-affiliated Phoenix Children’s Hospital (Arizona) and Nemours Children’s Health (Florida, Delaware, New Jersey, Pennsylvania). Clinicians included physicians (staff physicians, fellows, residents), nurse practitioners, physician assistants, and midwives (registered nurses only) in departments of family medicine, obstetrics/gynecology, primary care pediatrics, neonatology, and newborn nursery. Clinicians were included if they endorsed caring for healthy infants, postpartum mothers, or both groups and had provided direct patient care within the past year.
To obtain the perspectives of clinicians with special interest in vitamin D supplementation, surveys were also sent to pediatric endocrinologists and members of several international vitamin D and rickets working groups.12,19,23 In addition, members of a private social media group for physicians who are currently or planning to practice lactation medicine were invited to participate. This group includes more than 3000 members, all whom were vetted to verify physician status. Administrators of the group approved posts advertising the study with links to the survey.
Data Collection
Between April and August 2021, an e-mail invitation that included a brief description of the study, information about the estimated length of time of the survey, data storage, and the investigator team, and a link to the anonymous survey was distributed. Reminder e-mails were sent 2 weeks and 1 week before the survey closed 1 month after the initial e-mail. For the social media recruitment, 2 posts advertising the study with a link to the survey were posted approximately 3 weeks apart in April and May 2021. Data were kept on a password-protected, secure server accessible only by authorized study personnel.
Data Analysis
Survey responses were electronically collected and managed in Qualtrics. Data were summarized using frequencies and percentages for categorical data and medians and interquartile ranges (IQR) for continuous data. Comparisons were made between groups using Kruskal-Wallis tests for continuous and ordinal variables and either chi-square or Fisher’s exact tests for categorical data. For survey questions with 3 or more answer choices where each individual answer option was analyzed separately, p-values were adjusted for multiple comparisons using the false discovery rate method. Statistical analyses were performed using SAS version 9.4 software (SAS Institute, Inc.; Cary, NC).
Results
A total of 516 clinicians completed the survey. The exact number of individuals who received the survey was not captured due to the use of social media as 1 means of recruitment, but 2325 clinicians were emailed the survey. Six clinicians were excluded for not having provided patient care in the 12 months leading up to the survey, 81 were excluded for not caring for healthy newborns and/or postpartum mothers, and 69 were excluded for not having a primary practice in family medicine, obstetrics/gynecology, primary care pediatrics, neonatology, or newborn nursery. In total, 360 clinicians met inclusion criteria. This included 168 IC and 192 MIC.
We did not observe significant differences between the IC and MIC groups regarding gender, age, years of training or practice, whether they provided breast milk to their own infants, whether they provided vitamin D supplementation directly or indirectly to their own infants, or the age of their youngest child. IC had proportionately fewer midwives, nurse practitioners, and physician assistants and proportionately more physicians. MIC were more likely to have received additional training in lactation medicine and to practice in the US and were less likely to have their own children (Table 1).
Demographic Features of Clinicians
IC were more likely than MIC to have seen at least 1 child with nutritional rickets (48.2 vs 4.2%, P < .001), to recommend vitamin D supplementation for the purpose of preventing rickets (61.1 vs 32.2%, P < .001), and to have seen at least 1 child with vitamin D toxicity (11.9 vs 1.6%, P < .001). In their current practice, IC were more likely than MIC to recommend vitamin D supplementation to exclusively breastfed infants (P < .001, median 100 (IQR 100-100), median 98 (IQR 90 to 100), respectively) and to partially breastfed infants or infants receiving less than 1000 mL of formula daily (P = .005, median 90 (IQR 60.5 to 100), median 80 (IQR 30 to 100), respectively). MIC were more likely than IC to recommend vitamin D supplementation to breastfeeding mothers via a prenatal vitamin only (10.8 vs 1.8%, P < .001), which does not contain enough vitamin D to sufficiently meet the needs of an infant, and to discuss infant and maternal supplementation options and let the parents/caregivers choose (34.7 vs 22.0%, P = .009) (Table 2).
Current Vitamin D Supplementation Prescribing Practices of Infant-Only Clinicians and Clinicians Who Care for Mothers and Infants
If supplementing the mother with high-dose vitamin D or the infant directly each provided adequate vitamin D status in the infant and both were safe, MIC were more likely than IC to think that supplementation of the mother would be preferred by most parents/caregivers (63.0 vs 45.2%, P = .003), lead to greater adherence (66.5 vs 49.4%, P = .006), and promote breastfeeding (54.7 vs 36.5%, P = .001). In contrast, IC were more likely than MIC to think that supplementation of the infant would be preferred (14.9 vs 7.3%, P = .048). In this scenario, both MIC and IC indicated they would be most likely to offer both options and let the parents/caregivers decide (70.3 vs 69.6%, P = .98). MIC would be more likely than IC to recommend supplementation of the mother (17.7 vs 8.9%, P = .04); IC would be more likely than MIC to recommend supplementation of the infant (21.4 vs 12.0%, P = .04) (Table 3).
Vitamin D Supplementation Prescribing Preferences of Infant-Only Clinicians and Clinicians Who Care for Mothers and Infants
Among clinicians in both groups, in their current practice, female clinicians (27.7 vs 7.9%, P < .001), clinicians with additional training in lactation medicine (53.4 vs 16.9%, P < .001), clinicians with children (25.7 vs 13.2%, P = .02), and clinicians who supplemented their own children (30.5 vs 15.2%, P = .01) were more likely to recommend vitamin D supplementation to breastfeeding mothers at doses higher than a prenatal vitamin. Female clinicians (34.1 vs 9.2%, P < .001) and clinicians with additional training in lactation medicine (60.3 vs 22.2%, P < .001) were also more likely to discuss infant and maternal supplementation options and let the parents or caregivers choose. Clinicians who had supplemented themselves or their partners for the purpose of supporting their infant’s supplementation needs were more likely to recommend vitamin D supplementation to exclusively (P < .001, median 100 (IQR 100-100), median 98 (IQR 70 to 100), respectively) and partially breastfed infants (P < .001, median 90 (IQR 62 to 100), median 70 (IQR 25 to 98), respectively) than clinicians who did not supplement themselves or their partners with vitamin D.
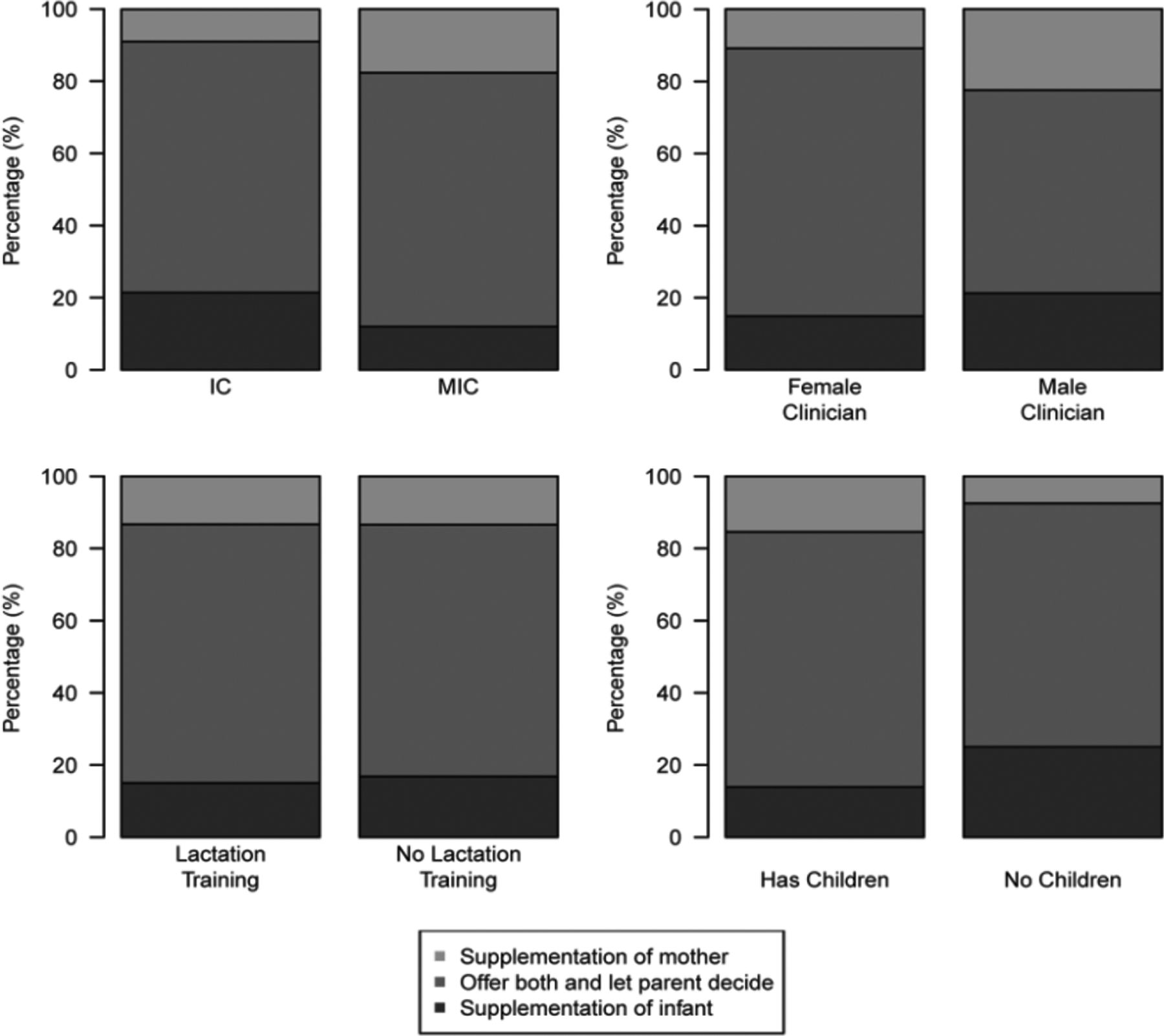
If supplementing the mother with high-dose vitamin D or the infant directly each provided adequate vitamin D status in the infant and both were safe, female clinicians would be more likely than male clinicians to offer both options and let the parents or caregivers choose (74.3 vs 56.3%, P < .001) (Figure 1).

Proportion of Clinicians Who Would Recommend High-Dose Vitamin D Supplementation of the Mother, Direct Supplementation of the Infant, or Both Options If Each Provided Adequate Vitamin D Status in the Infant and Both Were Safe. Abbreviations: IC, infant-only clinicians; MIC, mother-and-infant clinicians.
Pediatric endocrinologists were surveyed, however only twelve met inclusion criteria, because others answered “no” when asked if they care for healthy newborns and/or postpartum mothers. Therefore, pediatric endocrinologists were excluded from the main analysis.
Discussion
Our study revealed important differences between current infant vitamin D supplementation recommendations of MIC and IC. We also observed contrasting perspectives regarding high-dose maternal vitamin D but noted that both groups were open to offering this option if safe and effective.
In our study, IC endorsed higher rates of recommending supplemental vitamin D to exclusively and partially breastfed infants compared with MIC (Table 2). Among those who did not prescribe vitamin D to all infants for whom it is indicated, the most common specified reason was lack of awareness regarding guideline recommendations (Table 2). Scope of practice may have influenced our results as some clinicians in the MIC group may be less familiar than IC with AAP guidelines. Although obstetrics/gynecology clinicians care primarily for the mother, the American College of Obstetricians and Gynecologists does recommend discussion of infant care and feeding at the postpartum visit.24 The American Academy of Family Physicians does not have an official clinical recommendation or guideline on infant vitamin D supplementation, which may further limit MIC understanding of the importance of supplementation. In a study among military pediatricians and family medicine physicians, the most common reason for not recommending vitamin D was the belief that breastfed infants receive adequate sunlight exposure.25 In comparison, just 2 clinicians out of 360 in our study advised regular sunlight exposure instead of vitamin D supplementation (Table 2). Previous research found that 70% of family medicine clinicians reported recommending supplemental vitamin D to exclusively breastfed infants and 54.3% recommended it to partially breastfed infants.22 Both IC and MIC in our study indicated that following guidelines was the primary reason they recommend supplementation, highlighting the importance of guideline recommendations.
Overall, both groups endorsed high rates of recommending supplemental vitamin D to infants (Table 2). Although 93.6% of clinicians in our study stated they recommended vitamin D supplementation to follow guideline recommendations, we found that certain groups were more likely to follow these guidelines, specifically individuals who had supplemented themselves or their partners for the purpose of supporting their infant’s vitamin D needs and IC. IC were also more likely to have seen cases of rickets (Table 2). Nutritional rickets still occurs in the United States and is an entirely preventable disease.8 Furthermore, AAP guidelines and Global Consensus recommendations support universal supplementation.9,19 Our findings suggest that, despite a collective desire to practice guideline-informed medicine, personal experience also influences clinicians’ practices.
Clinical practice that includes mothers may also influence perspectives on supplementation options. MIC embrace maternal choice in infant vitamin D supplementation more so than IC. In their current practice, MIC were more likely than IC to give parents/caregivers the option to choose infant or maternal supplementation (Table 2). We previously found that family medicine clinicians would prefer to offer both options or maternal supplementation over infant supplementation alone.22 This highlights an opportunity to educate IC about this option, which may be less familiar to them. Encouragingly, if each option provided adequate vitamin D status in the infant and were safe, both groups indicated that they would offer both choices and let the parents or caregivers decide (Table 3).
Maternal vitamin D supplementation was favored by female clinicians, clinicians with additional training in lactation medicine, clinicians with children, and clinicians who supplemented their own children. These individuals may share insight into challenges with administering infant vitamin D drops or the potential advantages of maternal supplementation. Most clinicians (54.7%) in our study thought that high-dose maternal supplementation would be preferred by parents/caregivers if it were safe and effective (Table 3). This is likely an underestimate, as a similar survey of breastfeeding mothers showed that 88.4% preferred to supplement themselves rather than their infants.26
In addition to providing greater choice to the mother, potential benefits of high-dose maternal supplementation include promotion of the complete nutritional value of breastfeeding for infants, avoidance of potential vitamin D toxicity from incorrect dosing of infant drops, and possibly improved adherence to supplementation guidelines. In addition, maternal vitamin D status is related to breast milk composition and improved immunologic markers in their infants.27
Numerous studies have shown that high-dose maternal supplementation is a safe and effective way to raise 25-hydroxyvitamin D (25(OH)D) levels in mothers and the breastfeeding infant.11,14⇓–16 Maternal intake of a single oral dose of 150,000 IU (3750 mcg) of vitamin D3 increased infant mean serum 25(OH)D (± standard deviation) from 17 ± 13 to 39 ± 6 ng/mL (to convert to nmol/L, multiply by 2.496) after 1 month; infants whose mothers received 5000 IU (125 mcg) per day for 28 days had a similar increase from 16 ± 12 to 39 ± 12 ng/mL.14 Infants whose lactating mothers received 6400 IU (160 mcg) of vitamin D3 per day achieved equivalent vitamin D status compared with infants who were directly supplemented with 400 IU (10 mcg) per day and whose mothers received 400 IU (10 mcg) per day.15 Finally, infants of mothers who received 4000 IU (100 mcg) per day for 3 months had increases in serum 25(OH)D from a mean (± standard error of the mean) of 13.4 ± 3.3 to 30.8 ± 5.0 ng/mL.16 Given recommendations that healthy individuals maintain 25(OH)D levels of at least 20 ng/mL to achieve vitamin D sufficiency and prevent rickets,18,19 these studies highlight several potential dosing options for maternal high-dose vitamin D supplementation.
Vitamin D toxicity in children is rare, but it is not merely a theoretical risk, as 11.9% of IC and 1.6% of MIC had encountered children with vitamin D toxicity (Table 2). Although the incidence of hypervitaminosis D among individuals of all ages increased significantly from 2002 to 2011 in a population-based study in Olmsted County, Minnesota, this increase was not associated with clinical vitamin D toxicity.28 Nonetheless, the traditional supplementation method of giving vitamin D directly to infants carries risk of vitamin D toxicity secondary to dosing errors (drops vs mL), poor quality control regulation of supplements, and accidental ingestions.29⇓⇓–32 Supplementation of the mother may be a more reliable means of avoiding the risk of vitamin D toxicity for breastfed infants.
There were several limitations to our study. First, the survey was not tested for validity or reliability, and we were unable to determine the exact response rate due to use of social media. Another limitation was the potential for recall bias among clinicians who may have inaccurately reported their prescribing practices. Lastly, although we surveyed clinicians from diverse geographic locations and practice types, our survey used a convenience sample, and therefore, those who responded to the survey may not represent those who chose not to complete the survey or who work in other regions or practice settings, thus limiting its generalizability.
Both IC and MIC recommend infant vitamin D supplementation at high rates, yet neither group fully met the AAP guideline. MIC are more likely than IC to embrace high-dose maternal vitamin D supplementation to provide adequate vitamin D for breastfed infants. Nonetheless, both groups expressed openness in this option. We recommend that the American Academy of Family Physicians consider publishing a clinical recommendation on infant vitamin D supplementation, including the option of high-dose maternal vitamin D supplementation, given poor adherence to existing guidelines.
Appendix

Notes
This article was externally peer reviewed.
Funding: This study was supported by the Mayo Clinic Parker D. and Isabella G. Sanders Endowed Professorship in Family Medicine.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/1/95.full.
- Received for publication July 17, 2022.
- Revision received September 24, 2022.
- Accepted for publication September 27, 2022.




{kind=link}