
Abstract
Background: With the goals of improving health care delivery, patient outcomes, and creating a more engaged workforce, there have been consistent calls over the past 2 decades for increasing research capacity within the field of family medicine. Since 2014, the University of Minnesota Department of Family Medicine and Community Health (UMN DFMCH) has implemented strategies to enhance clinical faculty research capabilities while maintaining high-quality clinical care and medical education. This study reports changes in clinical faculty publications.
Methods: Peer-reviewed publication data from 2013, 2016, 2019, and 2022 were analyzed for clinical faculty employed by the UMN DFMCH during those years. An annual research culture survey was administered via e-mail to clinical faculty in 2021, 2022, and 2023. The survey asked questions regarding Research Leadership, Culture, Training, Infrastructure, and Capacity.
Results: While 2019 had the highest total number of publications with 99, 2022 had the highest proportion of faculty with at least 1 publication (50%). In 2023, 63.6% of survey respondents thought there were opportunities for them to participate in research, up from 41.0% in 2021. When asked about their research capacity and goals, 43.5% in 2023 responded positively, compared with 19.4% in 2021.
Conclusions: The efforts in our department to increase research capacity through investing in research infrastructure, faculty training and mentoring, and funding have led to notable increases in clinical faculty publications and positive perceptions of our research culture. These results provide additional evidence of the value of a model that harmonizes clinical care, education and research missions.
- Bibliometrics
- Delivery of Health Care
- Family Medicine
- Leadership
- Medical Education
- Medical Faculty
- Research Capacity Building
- Scholarships
- Surveys and Questionnaires
- Workforce
Introduction
Twenty years ago an international group of family medicine scholars identified increasing primary care research as critical to improving population health globally.1 This group proposed that increasing research capacity within the field of family medicine would lead to improved health care delivery, patient outcomes, and a more engaged workforce - a premise that has subsequently been reiterated by other scholars.1⇓–3 Family medicine clinicians, particularly those in academic settings, experience limited research infrastructure and funding support and competing priorities: clinical care and medical education.3⇓⇓⇓–7 These barriers to conducting research can interfere with the success of family medicine clinicians seeking promotion and/or tenure.8
Three United States-based national organizations (North American Primary Care Research Group (NAPCRG), Society of Teachers of Family Medicine (STFM), and the Association of Departments of Family Medicine (ADFM)) have developed joint initiatives to expand the capacity for family medicine research.3,9,10 Since 2015, these collaborations have resulted in new research training opportunities, greater dissemination of research through family medicine journals and conferences, and additional federal funding focused on family medicine research. In addition, experts from these organizations have compiled evidence-based recommendations for building capacity to conduct research in family medicine.10
The efforts over the last twenty years to increase family medicine research capacity have largely made an impact, with observed increases in publications by family medicine faculty,11,12 cultural shifts within department leadership toward favoring research,13 and self-described “high capacity” for research among many family medicine departments.14 With respect to family medicine departments, previous studies have identified, at a high level, which features may be associated with improving research capacity.13,15,16 Among the most impactful changes were standardized mechanisms for training faculty in research skills and grant writing and connecting them with a PhD research mentor. At the 2023 NAPCRG Research Summit, concrete plans for advancing family medicine research capacity were identified, including strategies to enhance infrastructure, training/mentoring, and advocacy/funding. Given these newly revived efforts to reach the goal of increasing research capacity within family medicine departments in academic medicine, models of successful programs are needed.
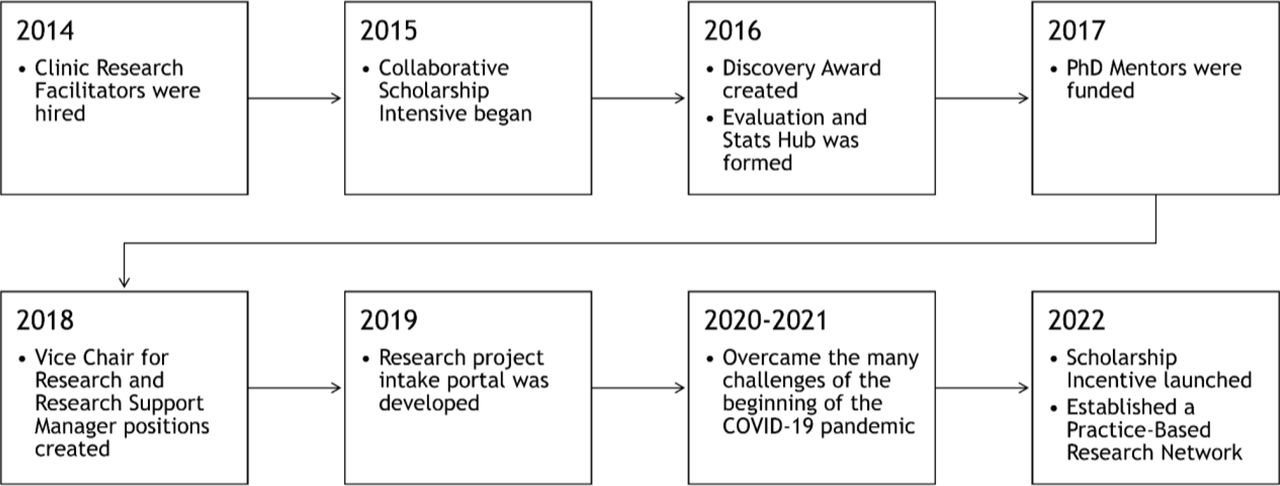
Since 2014, the University of Minnesota Department of Family Medicine and Community Health (UMN DFMCH) has made concerted efforts to increase faculty research capacity, without disrupting exceptional clinical care and medical education.16,17 (Figure 1) Described in more detail previously,16 the most notable actions taken by UMN DFMCH include (1) hiring research support staff, (2) offering structured training and mentoring opportunities, (3) administrative leadership roles for research, (4) research-focused career pathway opportunities, and (5) increasing research funding. As of 2023 the research infrastructure included 5 clinic-based research facilitators to assist with study start-up, recruitment and implementation, evaluation and statistical support from a full-time biostatician and 2 part-time PhD research mentors, grant writing and regulatory assistance, and an annual faculty scholarship course, the Collaborative Scholarship Intensive.17 Our transformation consisted of an ensemble of highly interrelated changes or strategies developed iteratively over several years. It was designed not as separate strategies with separate effects, but as 1 multi-dimensional strategy related to what we have previously published as “harmonizing the missions.”18 In 2016, UMN DFMCH also created an annual funding mechanism for clinical faculty, the Discovery Award, which supports early stage ideas, creative research, and scholarly projects that advance the art and science of family medicine. The department also started offering a yearly publication salary incentive in 2022. Clinical faculty were eligible to receive a financial “scholarship incentive” if they were a coauthor on a submitted manuscript, or grant proposal. Receiving grant funding or having the manuscript accepted for publication were not requirements for the incentive.

Timeline of the implementation of research infrastructure in the University of Minnesota Department of Family Medicine and Community Health between 2014 and 2022.
These changes were made with the support, and in support of, the clinical care and education pillars of the department. The main aim of the present study is to evaluate the growth in research capacity and culture of the UMN DFMCH, via 10 years of publication metrics and 3 years of longitudinal faculty survey results focused on the research culture. Our findings also provide a concrete example for how to evaluate research capacity within a department of family medicine within academic medicine.
Methods
This study analyzed peer-reviewed publication data for clinical faculty employed by the UMN DFMCH in 2013, 2016, 2019 and 2022. These years provided a baseline (2013) and ongoing snapshots of scholarship since UMN DFMCH began investing in research transformation in 2014. The UMN DFMCH launched an annual research culture survey in 2021.
Population
Our study population was UMN DFMCH clinical faculty of 4 family medicine residency clinics or practicing in 3 primary care clinics in Minneapolis and St. Paul, Minnesota. During the study period, the number of faculty ranged from 69 in 2013 to 81 in 2019 and included interprofessional providers such as physicians, nurse practitioners, pharmacists, and behavioral health clinicians. The current study included all UMN DFMCH clinical faculty with <= 30% academic research/scholarship time. Excluded from the study were MD and PhD research faculty (ie, faculty with >= 70% research/scholarship time) with minimal or no clinical role.
Publication Data
Publication data for clinical faculty for the years 2013, 2016, 2019 and 2022 were obtained via an internal platform that pulls information directly from the Scopus database (Scopus, Elsevier). Publications were included if a clinical faculty was an author of a print or online article published in a peer-reviewed journal. Only original research articles, systematic reviews and research briefs (or equivalent) were included. Commentaries, essays and other short form articles were excluded. Articles considered “in press” as of July 2023, were also excluded. The variables extracted for each publication included the article title, author list, journal name, date of publication and 2022 Journal Impact Factor (Clarivate Plc). Publications were matched to clinical faculty and an annual count of publications and first authorships were determined for each faculty member.
Research Culture Survey Process
Longitudinal surveys were administered to faculty via e-mail in October 2021, June 2022 and June 2023, using the University of Minnesota’s Research electronic data capture (REDCap) platform.19 Participants received 4 reminders, sent biweekly following the initial survey invitation. The survey was adapted from the research capacity and culture tool developed by Holden et al.20 and included 38 questions across 8 domains: Leadership Vision, Culture of inquiry, Research Training, Research Infrastructure, Externally Funded Research, Community-Engaged Research, Research Participation, Research Capacity. The present study focused on the Leadership, Culture, Research Training, Research Infrastructure and Research Capacity Domains. Questions were asked on a 5-point Likert scale, from Strongly Disagree to Strongly Agree, or Never to Very Often.
Statistical Analysis
Publication data were summarized by year with descriptive statistics to determine the total number of publications, number of authors per publication, the proportion of faculty with at least 1 publication and the proportion of faculty with at least 1 first author publication. The number of publications per journal was summarized across all 4 time points. The mean and range of 2022 Journal Impact Factors were calculated for the 10 journals with the most publications across all 4 time points. Among faculty present at all 4 time points, a Friedman test was conducted to identify any differences in annual publications by faculty member, and Cochran's Q test was run to determine if the proportion of faculty with at least 1 publication differed between time points. Post hoc analyses included pairwise comparisons, with a Bonferroni correction for multiple comparisons. Survey data were dichotomized into positive (Strongly Agree or Agree; Very Often or Often) and neutral/negative groups, and summarized using descriptive statistics.
This study was reviewed by the University of Minnesota Institutional Review Board and determined to be Not Human Research.
Results
The number of unique journals clinical faculty were published in across all 4 time points was 125, with 6 (4.8%) identified as journals specific to family medicine. Clinical faculty primarily published in journals that focused on research in the areas of family medicine care delivery, family medicine education, sports medicine research, clinical pharmacy, sexual and gender health and geriatrics. The 20 journals that had the most publications across all 4 time points accounted for 51.2% (n = 127) of all publications (n = 248).(Table 1) All 4 years included publications in Evidence-Based Practice, and 3 years included publications in Current Sports Medicine Reports, Academic Medicine, American Family Physician, and Clinical Journal of Sports Medicine.
The 20 Journals with the Most Publications Across All 4 Years: 2013, 2016, 2019, and 2022
Table 2 shows the increase in publications among clinical faculty between 2013 and 2022. While 2019 had the highest total number of publications with 99, 2022 had the highest proportion of faculty with at least 1 publication (50%). Among clinical faculty who were members of the department at all 4 timepoints (n = 34), both the total number of publications and proportion of faculty with at least 1 publication increased over time. (Table 3) The median number of authors per publication varied across time points for both groups, but similar medians and interquartile ranges were observed.
Publication Among All University of Minnesota Department of Family Medicine and Community Health Clinical Faculty, 2013–2022
Publication Among University of Minnesota Department of Family Medicine and Community Health Clinical Faculty Who Were Members of the Department at All Four Timepoints (n = 34), 2013–2022
Among all faculty, the proportion with at least 1 publication was significantly different across timepoints (χ2(3) = 8.833, P = .032). Pairwise comparisons using Dunn’s procedure determined there was only a statistically significant increase (adjusted P = .023) between 2013 and 2022. The proportion of faculty with at least 1 first author publication did not differ significantly between time points. While annual publications by faculty members significantly differed over time (P = .008), post hoc analysis did not identify any significant differences between specific time points.
Response rates to the research culture survey were consistently high: 62/72 (86.1%) in 2021, 63/76 (82.9%) in 2022 and 69/76 (90.1%) in 2023. Overall, clinical faculty perception of the research culture has improved since 2021. (Table 4) 72.5% of respondents in 2023 considered leadership to be supportive of clinician research, compared with 61.3% in 2021. In 2023, 63.6% thought there were opportunities for them to participate in research, up from 41.0% in 2021. Perceived availability of research mentoring also increased, from 61.3% in 2021 to 84.1% in 2023. Regarding research infrastructure, in 2021, 63.9% of faculty responded positively about the availability of resources to support research, which increased to 87.0% in 2023. When asked about their research capacity and goals, 43.5% in 2023, compared with 19.4% in 2021, were meeting their research goals, and satisfied with their capacity.
University of Minnesota Department of Family Medicine and Community Health Clinical Faculty Perceptions of the Department Research Culture Across 5 Domains, Proportion of Positive Responses, 2021–2023
Discussion
Since 2013 there has been a noticeable increase in scholarly output by clinical faculty within the UMN DFMCH. In 2022 (which included the COVID-19 pandemic years), 50% of DFMCH clinical faculty members published at least once, which is markedly higher than what has been observed nationally: 15% in a 2019 study using 2015 data.11 The number of faculty with 2 or more publications also increased, nearly doubling between 2013 and 2022. While most of the publication metrics had notable increases, the proportion of faculty with at least 1 first authorship only increased modestly, and the median number of authors both increased and decreased over time. In alignment with the demands of being a primarily clinical faculty in family medicine, our results suggest that the majority of our clinician faculty increased their research output by joining as coauthors on articles. This may be one way to increase clinical faculty publications that other institutions could replicate. Connecting primarily clinical faculty with other faculty engaging in research to collaborate on publications can balance the time-prohibitive nature of conducting primary data collection alongside clinical responsibilities.
The observed growth in scholarly output aligns with the increasingly positive research culture survey, which also showed noticeable improvements across just a few years. While the transition to a robust infrastructure in the department was incremental, the majority of the research infrastructure supporting faculty was in place by 2020. Our data suggest that the impact of such an infrastructure continues to grow years beyond implementation, which speaks to the importance of department culture and values. A majority of faculty reported increasing perceptions of access to research mentoring and coaching and career pathways available to those who want to emphasize research and scholarship over time – important components of prior family medicine research model pathways.13,21 Training provides clinicians who may not have participated in research previously a supportive environment to learn, while career pathways provide clinicians who are experienced in research the opportunity and time to pursue a hybrid clinician-researcher career. Another finding was the consistently positive responses across the Leadership and Culture domains. These findings suggest that faculty know that publications are strongly encouraged, as well as incentivized, that they feel supported by department leadership, and that they perceive that research is embedded into the culture, all key attributes of a successful research department.13
While a majority of the questions had a high proportion of positive responses when the survey was first administered in 2021, those within the Research Capacity domain were relatively low and continued to be in 2023. Notably, less than half (43.5%) of the clinical faculty thought their current capacity to participate in research matched their goals. The survey did not explore barriers to research participation. However, the literature suggests that the competing priorities of clinical care, education and research often lead to the least urgent priority–research–to be postponed.16 While protected research time has long been proposed as a solution, it is constrained by ever increasing clinical care demands and limited faculty administration time. Faculty in our department without grant funding have 20% administration time for charting, educational endeavors, committee work and research/scholarship. Collaborating on research projects rather than conducting original programs of research might be a more feasible pathway to research participation for clinical faculty operating within these constraints.
Clinical faculty generally published in the same set of journals across the 4 time points. A smaller subset were in typical family medicine journals. Our results align with national data, which found that in 2015, 84% of the journals family medicine faculty were published in were nonfamily medicine journals.11 This breadth of publishing outside of family medicine specific journals reflects the nature of family medicine, an all-encompassing specialty, and one of the challenges the field faces while trying to create a research identity.7The present study has several limitations. Due to the longitudinal nature, this study was only able to provide a high-level evaluation of the publication data and not a comprehensive bibliometric analysis. It was unable to discuss research output measures that extend beyond the quantity of publications, such as authors’ h-index, journals’ impact factor, citation-related metrics, or network analyses. The study is also limited by the publication data, as it was extracted from a single major research database–Scopus. Any publications not included in the Scopus database would have been missed and not included in the analysis. This study was also focused on a single institution and its research infrastructure and faculty, making the findings less generalizable than a multi-site study. Given the simultaneous implementation of our intervention components and their iterative nature over this study time period, we are unable to disentangle the influence of the individual components, attribute outcomes to a specific component, or examine interaction effects. While this is not a limitation in approach, it limits our ability to describe the timeline and makes it more challenging for others to mimic our efforts. Further, the study was limited by the nature of voluntary self-reported surveys. Although response rates exceeded 80% each year, it is unclear why some faculty did not complete the survey. Lastly, the subjective nature of some of the survey questions may have contributed to different interpretations by respondents.
The efforts in our department to increase research capacity through investing in research infrastructure, faculty training and mentoring, and funding have led to notable increases in clinical faculty publications and positive perceptions of our research culture. These results provide additional evidence of the value of a model that harmonizes clinical care, education and research missions.
Acknowledgments
This study was supported by the Research Services Hub, in the Department of Family Medicine and Community Health, University of Minnesota Medical School.
Notes
This article was externally peer reviewed.
Conflict of interest: The authors have no conflicting or competing interests to declare.
Funding: This project was not funded by any grants or external agencies.
To see this article online, please go to: http://jabfm.org/content/37/6/1047.full.
- Received for publication February 9, 2024.
- Revision received April 26, 2024.
- Accepted for publication May 13, 2024.




{kind=link}