
Abstract
Background: Transgender and nonbinary (TGNB) patients face significant health disparities and negative experiences in health care spaces. With our family medicine residency clinic caring for an increasing number of TGNB patients, we sought to better understand the unique experiences and needs of this population.
Methods: We utilized a mixed methods approach, recruiting participants via our online patient portal and inviting them to complete a 36-item online survey and/or participate in one of four 90-minute focus groups exploring their interactions with a variety of care team members, perspectives on our physical clinic space, ideas for improvement, and other areas. We analyzed survey data using descriptive statistics and performed open coding on survey free-text responses and interview transcripts to identify salient themes.
Results: 90 TGNB patients completed the survey, and 20 participated in the focus groups. Participants described a variety of positive interpersonal and noninterpersonal experiences including being gendered correctly, clinicians being knowledgeable and responsive to feedback, and seeing visible markers of LGBTQ+ inclusivity. Negative experiences included misgendering and deadnaming, being asked unnecessary questions, and being outed as TGNB without their consent.
Conclusions: Participants’ positive and negative health care experiences, along with their specific recommendations for interpersonal and system-level change, will help guide ongoing efforts to improve the care of TGNB patients at our clinic. Future needs assessments and ongoing conversations with our TGNB patients are needed to further explore this study’s emerging themes, with particular attention to the impact of age, race/ethnicity, primary language, and other intersecting identities on TGNB patient experiences.
- Access to Care
- Community Health Care
- Community-Based Participatory Research
- Family Medicine
- Focus Groups
- Gender-Affirming Care
- Health Disparities
- Health Equity
- LGBTQ
- Minority Health
- Patient Participation
- Primary Health Care
- Qualitative Research
- Surveys and Questionnaires
- Transgender Persons
Introduction
Compared with the general population, Transgender and Nonbinary (TGNB) individuals shoulder a disproportionate burden of chronic stress, housing instability, and emotional, physical, and sexual violence.1⇓⇓–4 This burden contributes to a wide range of physical and mental health disparities, including but not limited to higher rates of depression, suicidal ideation and attempt, substance use disorder, eating disorders, and sexually transmitted infections among TGNB individuals.2,3,5 This population also faces barriers to consistent health care access, including financial instability and lack of insurance, as well as negative health care experiences ranging from implicit bias and insufficient clinician knowledge to experiences of overt discrimination.6⇓⇓–9 In a 2015 national survey, one third of TGNB respondents reported at least one negative experience within the past year related to their TGNB identity when seeking health care, with nearly a quarter reporting avoidance of medical care due to fear of mistreatment.10 Considering the well-documented role of continuity of care in chronic disease management, this avoidance of care likely contributes to the higher rates of obesity, chronic pulmonary disease, and other chronic conditions observed in TGNB individuals compared with their cisgender counterparts, a disparity that persists even among those with private health insurance.9,11,12
Health care systems can help break this harmful cycle of discrimination and avoidance through education, behavior, clinical practice, and culture change.6,13,14 To help inform these changes, several clinics have conducted needs assessments to better understand the experiences and needs of TGNB patients.15⇓–17 These assessments have identified multiple areas for improvement and growth, including a need for clinician and staff training around TGNB health and identities, more opportunities for patients to self-identify in clinical spaces (including name, gender identity, and pronouns), clarification around anatomy-specific screening protocols (eg, breast or cervical cancer screenings), and more accessible mental health resources.15⇓–17
Family Medicine residency clinics, particularly those housed within large academic health systems, are often sites of innovation in clinical education and practice. To date, however, the authors are aware of only one comprehensive needs assessment of TGNB patients at a family medicine residency clinic, published over six years ago.16 Given the many advancements and challenges in TGNB health over the intervening six years, an updated needs assessment presents a critical opportunity to engage patient perspectives, promote health equity, and improve quality of care. To this end, our team utilized a quality improvement approach in seeking to answer the questions: how would TGNB patients at our family residency clinic describe their own experiences of seeking and receiving care at our clinic? From scheduling their first appointment, to entering the waiting room, to interacting with clinical and nonclinical staff, which experiential details do our TGNB patients identify as positively or negatively impacting the quality of their care – and how may these details inform future quality efforts to improve our care of this population?
Methods
We took a thematic qualitative approach,18 aiming to identify recurring themes and commonalities throughout the health care experiences of TGNB patients receiving care at our institution’s large family medicine residency clinic, which comprises 34 faculty clinicians, 24 resident clinicians, and serves roughly 20,000 active patients (ie, those with at least one visit sometime in the past 18 months), at least 600 of whom identify as TGNB. We accomplished this goal through an explanatory sequential mixed methods study, first distributing and analyzing a predominantly multiple-choice survey of TGNB patients at our clinic, and then conducting focus groups with a subset of survey respondents to further explore and explain these results through a qualitative lens.19 Our research team consists of an attending physician, a resident physician, and two student research assistants, all whom happen to identify as LGBTQ+ and two of whom identify as TGNB. The University of North Carolina School of Medicine’s Institutional Review Board (IRB) determined the study to be a quality improvement project and thus IRB approval was not required.
Recruitment
We took a pragmatic approach to recruitment, identifying eligible participants through an Epic (electronic medical record) report of adult patients seen in our clinic by any resident or faculty provider during an eligibility period of April 2022 through June 2023, and who had previously received the diagnostic code of “Gender Dysphoria (ICD F64.0)” in a prior encounter (including encounters outside of the eligibility period). We selected this code, which encompasses all diagnoses relating to gender-affirming care (including “gender dysphoria,” “gender dysphoria in adult,” and “transgender person on hormone therapy”), given its widespread use by resident and faculty providers to code any clinical encounter involving gender-affirming care, including but not limited to the prescription of gender-affirming hormones (GAH). While this may exclude TGNB patients who receive some form of medical care but not gender-affirming care at our clinic, including those who have not disclosed their TGNB identity to a member of their care team, we estimate that this constitutes a relatively small subset of our clinic’s TGNB patients.
This report identified 302 eligible patients, 300 of whom had active Epic patient portal (MyChart) accounts. We sent these 300 potential participants a MyChart message with information about the study, containing an external, nonpersonalized link to an optional, anonymous, online survey, as well was a separate external, nonpersonalized link to a secure form where participants could voluntarily enter their contact information to learn more about an optional focus group. The focus group link was also included at the end of the survey; however, a participant’s contact information was not linked to their survey responses to maintain survey anonymity. Survey completion was not required for focus group participation, and vice versa. Neither the survey nor the focus group form was linked in any way to the patient’s medical record or MyChart portal.
Survey Design
Our team collectively designed an anonymous, 35-item Qualtrics survey consisting of three yes/no eligibility questions, four demographic questions, 17 questions regarding overall clinic experience, four questions regarding mistreatment and other negative experiences, two questions regarding specialty referrals, six questions regarding clinician interactions, and three questions regarding patient satisfaction and opportunities for improvement. We estimate that the survey takes approximately 10 to 15 minutes to complete. Participants provided informed consent electronically on the first page of the survey link, before initiation of the survey.
In addition to a review of current literature around gender-affirming care and TGNB patient experiences, we consulted two main sources in creating this survey: the “health care” section of the US National Transgender Survey, the largest national survey designed by and for TGNB people, and our home institution’s patient experience survey, which was designed by an independent patient experience company (Press Ganey) and is distributed to all patients seen at any clinic within our home institution, (including those receiving care at our clinic) via text message, e-mail, and/or mail following each health care encounter.10 The former utilizes multiple-choice questions, commonly yes/no questions, to assess the frequency of specific experiences and sentiments among TGNB respondents, to compare these frequencies to the general population.10 The latter utilizes multiple-choice Likert scales to assess patient satisfaction and quality of experience, often on a scale of “very good,” “good,” “fair,” “poor,” or, “very poor.”20
In addition, our survey’s final 2 questions, “How do you think [our clinic] could improve the care provided to Transgender and Nonbinary patients?” and, “Is there anything else you want to tell us about your experiences of receiving care at “(this clinic)” as a Transgender or Nonbinary person?” are not multiple choice, but instead provide a text box for free-response. In addition to the quantitative analysis of multiple-choice survey responses discussed above, we have combined these free-responses with focus group transcripts to form a final text dataset for thematic analysis (see below).
Quantitative Analysis
We analyzed demographic results using descriptive statistics for both survey respondents and focus group participants. Because the survey was anonymous, we cannot determine how many focus group participants also completed the survey, but we suspect there is significant overlap given our recruitment method. All individual survey questions were optional other than the 3 initial eligibility questions.
In analyzing our survey’s Likert scale responses, we assigned a score of 1 to 5 to each response on a scale of “very poor” (1 point) to “very good” (5 points), determined the mean for each question among all survey respondents, and multiplied these by 20 to arrive at a “participant mean” for each question. Because these questions were reproduced exactly from our home institution’s patient experiences survey, we were able to compare each question’s “participant mean” to our clinic’s reported average score for all patients (the “all-clinic mean”) using a single-sample t test. For each question, we also calculated the “top box percentage,” that is, the percentage of respondents who selected the highest possible score (“very good,” corresponding to a score of 5/5), and compared these to corresponding all-clinic percentages using a χ2 test.
Focus Group Design
Following completion and quantitative analysis of survey responses, two nonclinician team members, one of whom identifies as TGNB, jointly conducted four semistructured 90-minute focus groups with four to six participants each. These focus groups were intended to further explore many of the themes addressed through the survey, including patient comfort at our clinic site, experiences with misgendering, examples of feeling affirmed or unwelcome due to their gender identity, and ideas for improvement. Focus groups were confidential among participants and study personnel, and all participants used pseudonyms during the focus group. Participants were e-mailed an additional consent form to review and sign electronically before the start of each focus group. Participants were also e-mailed an optional, deidentified demographics survey to fill out following completion of the focus group, to allow for comparison of focus group demographics to survey demographics. Focus group participants received $50 compensation for their time. All focus groups were audio recorded and transcribed, and held within one month of each other.
Thematic Analysis
Following completion of focus groups, our team developed a preliminary codebook for use in thematic analysis, based on a collective review of our survey’s quantitative analysis, free-responses, and current literature. Two team members used this codebook to perform open thematic coding of focus group transcripts and free-text survey responses using Dedoose Online version 8.3 (SocioCultural Research Consultants, University of California, Los Angeles). We met regularly as a team to resolve coding discrepancies and update our codebook via constant comparative analysis. We then sorted codes into three groups based on frequency: low (zero to two applications throughout all transcripts/free text responses), medium (three to nine applications), and high (10 or more applications). We collectively reviewed these codes to identify emergent patterns and salient themes.
Results
Demographics
Our Epic report identified 302 eligible patients, 300 of whom had active MyChart accounts and received the survey and focus group invitations. Ninety completed the survey and 20 participated in the focus groups (30% and 6.7% response rates, respectively). Compared with the eligible patient pool, survey respondents were predominantly white and young, and fairly evenly distributed by gender identity (Table 1).
Participant Demographics
Quantitative Analysis: Highlighting Disparities in Patient Experiences
Most survey respondents report good or very good experiences interacting with clinicians (95%), learners (90%), medical assistants (85%), radiograph technicians (81%), lab technicians (81%), and front desk and scheduling staff (80%). Most survey respondents report that their assigned clinician knows “almost everything about trans health care,” (33%) or “most things about trans health care” (54%). Similarly, respondents rate the comfort of the reception area and clinic rooms fairly highly on a five-point Likert scale (mean, 4.28 and 4.4, respectively).
With this said, direct comparison of participant responses to all-clinic responses reveals significant disparities in patient satisfaction. Table 2 summarizes participant and all-clinic mean responses to five Likert questions taken directly from UNC Health’s Patient Experiences Survey. Compared with clinic-wide patient satisfaction data from July 2023, our TGNB survey respondents reported lower average scores for clinicians’ explanations about their problem or condition, and for concern the clinician showed for questions or worries (Table 2). “Top box” scores were also significantly lower for survey respondents for all five questions when compared with all-clinic percentages (Table 2). Furthermore, when asked about interactions specifically at our clinic, 18% of survey respondents report being misgendered “sometimes,” 8% “frequently,” and 1% “all the time.” 14% of respondents reported being called the wrong name “sometimes,” 4% “frequently,” and 1% “all the time.”
Comparison of Mean Patient Satisfaction Scores and “Top Box” Percentages Between Study Participants and General Clinic Population
These results are supported by many of the emerging themes throughout our focus group transcripts and survey free-responses, which we discuss in further detail below.
Thematic Analysis: A Conceptual Model
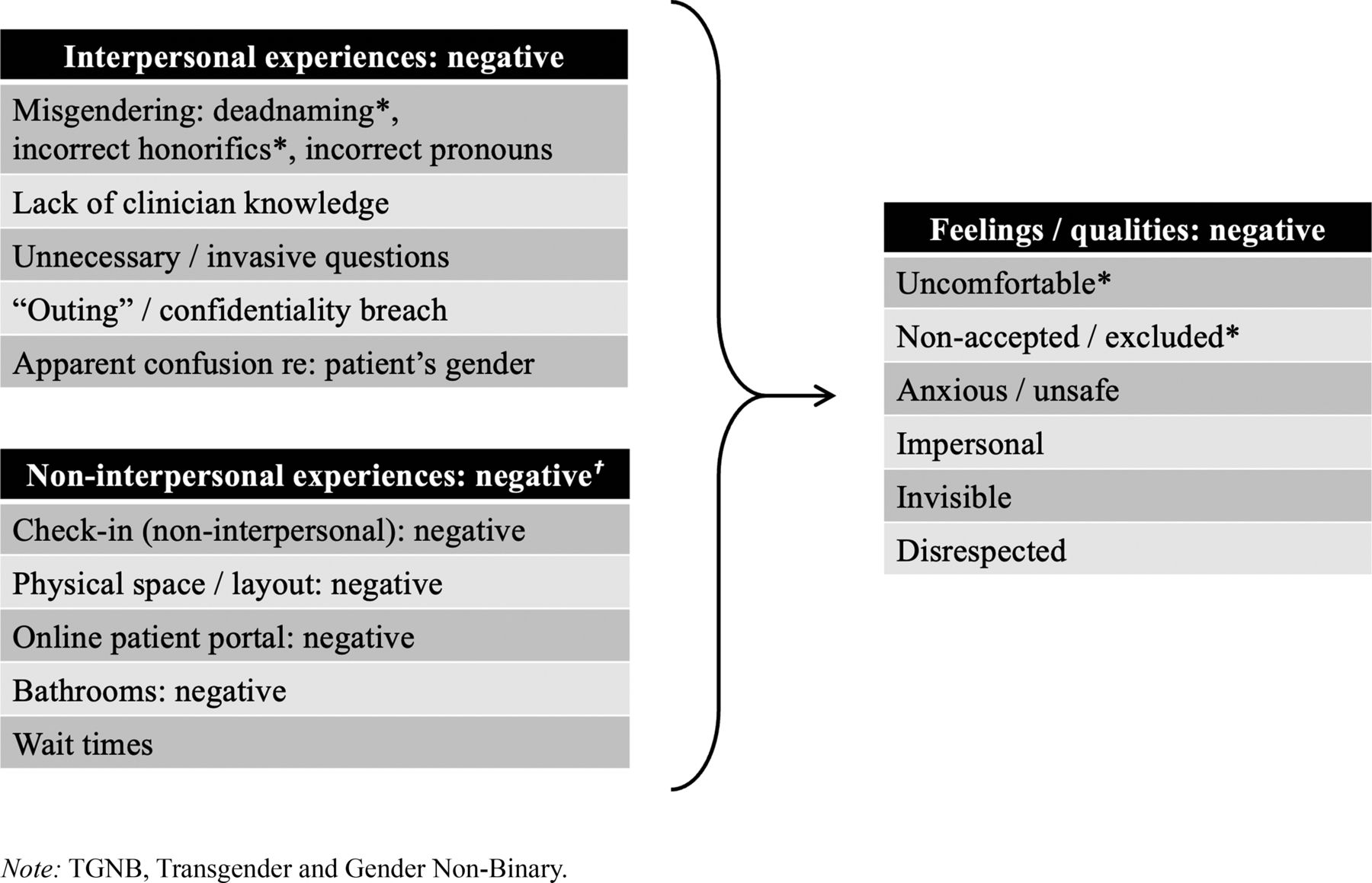
Following review of survey free-responses and two of four focus group transcripts, our team developed a list of 82 content codes for thematic analysis, with a kappa statistic of 0.80 reflecting excellent intercoder reliability. We divided these codes into two second-order themes: positive and negative experiences. Each of these was subdivided into three first-order themes: interpersonal, wherein participants describe specific interactions with clinical and nonclinical team members; noninterpersonal, wherein participants describe aspects of their clinic experience not involving direct interaction with a team member; and feelings/qualities, wherein participants describe the ways in which these experiences make them feel. We have arranged these themes into a conceptual model of TGNB patient experiences at our clinic, which we present in Figures 1 and 2.

Conceptual model of positive TGNB patient experiences. We have identified the most commonly occurring codes throughout all focus group transcripts and free-text survey responses and arranged these into a conceptual model of TGNB patient experiences at our clinic. Codes are presented in descending order of frequency. Those labeled with an asterisk (*) occur 10 or more times; all other codes occur between three and nine times throughout the dataset.

Conceptual model of negative TGNB patient experiences. Codes are presented in descending order of frequency. Those labeled with an asterisk (*) occur 10 or more times; all other codes occur between three and nine times throughout the dataset, with the exception of the codes listed under noninterpersonal experiences: negative (†), all which occur between one and five times.
Positive Experiences: Comfortable, Affirming, and Safe
Participants describe a wide range of positive interpersonal and noninterpersonal experiences, which help make them feel comfortable, safe, affirmed, understood, cared for, and invested in by their care teams (Figure 1).
Positive Interpersonal Experiences
Among both focus group participants and survey free-respondents, the most frequently noted positive interpersonal experience is that of being correctly gendered by a care team member (via chosen name or pronouns). One survey respondent writes, “My provider goes out of his way to use my name and pronouns in all communications that he can and answer any questions I have to reduce any anxiety.” Others highlight instances wherein a member of the care team incorporates their feedback or correction in real time, especially during instances of misgendering. When asked about “positive cues” indicating an affirming or safe clinic environment, one participant replies, “If they misgender me on the phone because they haven't heard my name yet, or something like that, and I correct them, and they [do not get] defensive. Just being like, ‘oh, okay!’ and moving on, and then not getting it wrong later.”
Participants also highlight clinicians demonstrating appropriate medical knowledge regarding gender affirming care, using appropriate anatomic terminology, and taking the time to explain important clinical concepts in patient-facing language. “one thing I really like about all the doctors I see,” reflects 1 focus group participant, “Is when they tell me, ‘okay, we're going to put you on this medication,’ and then they say, ‘and here's why.’…them taking the time to explain everything…that is so awesome.” Participants also highlight moments wherein team members demonstrate an investment in their needs, safety, and wellbeing. Describing an experience of checking into an appointment, one participant reflects, “The [nurse] that led me back, she asked me in the hallway where there was nobody else…‘do you feel safe at home?’…And that right there was like…wow, she really does care about my safety as a transgender person.”
Participants consistently characterize these experiences as making them feel comfortable, safe, invested in, and normalized in their gender experience. “For me,” reflects one participant, “I think what makes [an] affirming doctor, at the bare minimum, is just being willing to treat me as a person.”
Positive Non-Interpersonal Experiences
Participants also frequently comment on the positive impact of visual cues, signage, clinic layout, virtual check-in procedures, and other noninterpersonal experiences at our clinic. Describing the importance of seeing pronoun pins and pride paraphernalia on team members, one focus group participant explains, “I just needed to see that little reminder that it is okay that I exist, and that this person is okay with my existence, being who I am, and that I can openly and honestly say something to them.” Many participants specifically comment on the importance of virtual check-in kiosks and gender-neutral restrooms. One focus group participant explains, “I adore seeing gender neutral bathrooms…because it makes me feel like the people who designed the building… They knew that we existed. They had us in mind. It just makes us feel seen.”
Negative Experiences: Uncomfortable, Anxious, and Unsafe
Negative interpersonal and noninterpersonal experiences promote feelings of discomfort, anxiety, and even a lack of safety among survey free-respondents and focus group participants (Figure 2).
Negative Interpersonal Experiences
Reflecting on experiences that make them feel unwelcome, one survey free-respondent writes, “Being greeted as “sir” consistently in the waiting room, lab, by front desk staff, clinical staff, and technicians.” Citing frequent experiences of misgendering, particularly during phone interactions with administrative staff, many participants express a preference for scheduling and checking in via the online patient portal or check-in kiosks, rather than in-person or over the phone. “For me,” explains one focus group participant, “[Being misgendered] really encouraged me to find options that did not require interacting with people just with my voice. So, if there was like an online way to schedule things, that was usually what I would default to.”
Several participants also express concern regarding confidentiality, sharing instances wherein they were inadvertently “outed” (ie, revealed to be TGNB without their consent) by clinical or administrative staff. “Once,” reflects one focus group participant, “a lab tech started asking a lot of questions about being trans while she was drawing my blood. I hadn’t said anything related to my gender identity; she just saw it on my chart. She was not mean, just curious, but it was pretty uncomfortable because the door was open, and other people were walking by outside, and she was pretty loud.” Perhaps unsurprisingly, survey respondents demonstrate a strong preference for sharing their gender identity via the online patient portal (59%) or in a private interaction with their clinician (28%), rather than during the check-in (6%) or rooming process (7%). “I think the thing that I would like most,” reflects one focus group participant, “Is more privacy in every portion of the interaction…like [with] receptionists and [the] front desk and stuff…having that kind of insulation of like a more private space to have that conversation. As opposed to it just being out in the middle of everything, which is what makes that so, so miserable.”
While the majority of survey respondents indicate that their assigned clinician knows “everything” or “most things” about transgender health care, some focus group participants cite a lack of clinician knowledge around gender-affirming care, including expectations around surgical procedures and interpretation of sex-specific lab tests. Many also cite challenges with the availability and coordination of subspecialty referrals, including surgical and mental health care.
Negative Non-Interpersonal Experiences
Negative noninterpersonal experiences are much less frequently discussed than negative interpersonal experiences, with participants specifically noting the presence of gendered bathrooms, challenges with the patient portal, a lack of private space in the clinic outside of the examination rooms, and long wait times.
Discussion
Embracing the Positive: Affirming, “Whole-Person” Care for All
The results of this study highlight how both interpersonal and noninterpersonal factors shape the experience of TGNB adults receiving care in an academic family medicine setting. While some positive factors identified by participants are TGNB-specific, such as use of accurate name and pronouns, adequate knowledge about the care of TGNB individuals, and the presence of pronoun pins and other “safe space” signifiers, others are more broadly applicable, including the importance of mutual respect, attentiveness, longitudinal relationships, clinician-patient collaboration, patient-facing explanations, and responsiveness to feedback.16 Both focus group participants and survey free-respondents repeatedly share how these factors help them to feel safe, affirmed, and comfortable in clinical spaces.
These findings are consistent with previous TGNB patient experience studies, which have identified a welcoming clinical environment and “whole-person” clinical approach – defined by Hinrichs et al as considering each patient a “whole person with a full range of health needs, roles, identities, and experiences,” beyond simply their gender identity – as crucial to the wellbeing of TGNB individuals.16,23 Unfortunately, due to the systematic exclusion of TGNB experiences from clinical and professional education, many clinicians and staff members do not receive adequate exposure and training in the care of this population.21⇓–23 Clinic-wide trainings on respectful interaction with TGNB individuals, as well as more in-depth sessions catered to specific team roles, may help to harness and standardize these positive experiences – and, with time, promote a culture of respectful, affirming, “whole-person” care for all patients.
In addition to these previously identified factors, focus group participants and survey free-respondents also highlight several positive factors not addressed in prior studies, including the positive impact of our clinic’s online patient portal and electronic check-in kiosks. While our use of the patient portal for study recruitment likely biased our study population toward those who favor portal use, over 99% of all patients eligible for our study (adult patients seen in our clinic between April 2022 and June 2023 with “Gender Dysphoria (ICD F64.0)” on their problem list or as a visit diagnosis) have an active portal account, which is well above our overall clinic average. We look forward to further examining and optimizing the patient portal as a tool for advancing health equity and improving TGNB patient experiences in our clinic.
Learning from the Negative: Acknowledging Our Shortcomings to Build a Brighter Future
Survey respondents’ below-average patient satisfaction scores and “top score” percentages are likely related to misgendering, “outing”, invasive or unnecessary questions, inadequate clinician knowledge on TGNB health care, and other negative experiences shared by focus group participants and in free-text survey responses, as well as the resultant feelings of discomfort, invisibility, anxiety, or even lack of safety they describe. Many of these negative experiences are consistent with previous studies of TGNB individuals, which have enumerated the deleterious effects of misgendering, “outing,” and other forms of interpersonal and structural violence on this population.15⇓–17
As in previous studies, interactions with nonclinician staff (eg, lab, radiograph, and scheduling/front-desk staff) were rated the lowest by survey respondents.16 This may reflect a relative overconcentration of educational and other quality improvement interventions on clinicians, emphasizing the importance of including all members of the team in clinic-wide trainings and other efforts to improve the care of this population.
Participants also offer critical insight into challenges less often discussed in current literature, including concerns around “outing” in crowded clinic spaces and misgendering during phone interactions. These negative experiences may help to explain survey respondents’ strong preference for sharing their gender identity via the patient portal and positive response to our clinic’s recent adoption of virtual check-in kiosks, as well as the near-universal utilization of our online portal among TGNB patients. Altogether, these experiences invite a comprehensive review and revision of current clinic workflows, including implementation of gender-inclusive phone scripts and more widespread virtual options for scheduling, checking in, and indicating name and pronouns.15,16,24
Participant Recommendations: A Blueprint for Success
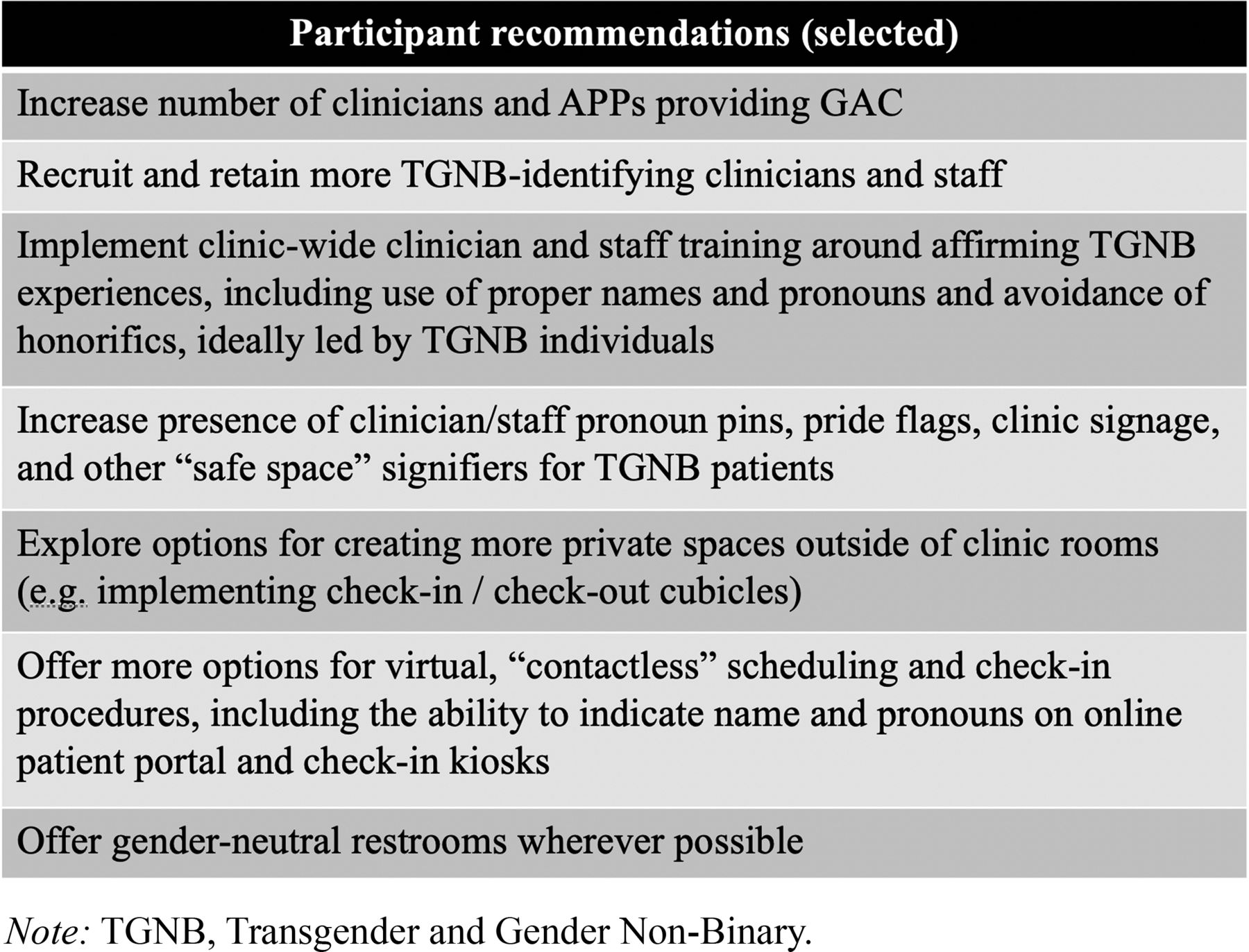
In addition to exploring their positive and negative health care experiences, this study was unique in explicitly asking focus group participants to provide recommendations for an “ideal” family medicine clinic experience. These recommendations encompass both interpersonal and systems-level interventions and are largely consistent with other study findings. We have summarized a selection of these recommendations in Figure 3. We hope they will serve as a blueprint for partnering with our TGNB patients to build a more inclusive, affirming clinical experience.

Selected participant recommendations. Participants recommend a wide range of interpersonal and systems-level interventions to improve the care of TGNB patients at our clinic, a selection of which are reproduced here. These recommendations are largely consistent with the major themes explored in Figures 1 and 2.
Limitations and Future Work
Generalizability of our results is limited by a lack of diversity among participants, particularly with respect to racial identity. 79% of all survey respondents and 90% of all focus group participants self-identify as White, compared with 68% of our clinic’s overall TGNB population. This discrepancy suggests a nonresponse bias that disproportionately centers White experiences, which is critical to consider in light of the deep racial/ethnic health disparities observed within the TGNB (and broader LGBTQ+) community.10 Future iterations of this project will prioritize outreach and accessibility to underrepresented subgroups within the TGNB umbrella, including those of racial/ethnic minority identities and those who speak a primary language other than English. Other limitations include likely overlap between focus group participants and survey respondents, recall bias, and potential for participant responses to reflect their health care experiences more generally and not exclusive to our clinic. Lastly, because it was compiled from other tools, our survey is not validated; with this said, we are unaware of a validated tool that would have addressed our stated aims as effectively.
Additional research is also needed to identify sustainable, evidence-based education tools for clinicians and staff to improve quality of care for our TGNB patients. In light of the relatively small percentage of primary care clinicians offering gender-affirming care – a barrier repeatedly cited by participants – interventions to recruit and train clinicians to offer these services are of particular importance. To this end, our residency program has begun developing and implementing a multifaceted approach to education on gender-affirming care for interested residents and faculty, for which preliminary outcomes have been promising.25 In addition critical are efforts to recruit and retain a gender-diverse health care workforce, including both clinical and nonclinical team members.
Lastly, while we present many of these findings as “novel” within the context of current medical literature, we must acknowledge TGNB communities' longstanding advocacy and health promotion work, much of which occurs outside of traditional clinical spaces. For decades, TGNB folks have responded to their negative health care experiences by engaging in knowledge sharing, intercommunity support, and advocacy on a local, national, and even international scale.26,27 With that said, this study is only a small part of what should be an ongoing conversation with our TGNB patients about their experiences and recommendations. We hope that our focus group study design will set the stage for ongoing patient involvement in gender affirming care at our clinic, including through a compensated community advisory board.
Conclusion
The provision of gender affirming care is rapidly expanding in family medicine residency programs and clinics. Our TGNB participants generously shared a wide range of positive interpersonal and noninterpersonal health care experiences, as well as resultant feelings of comfort, safety, investment, affirmation, and understanding. Many patients also shared negative health care experiences, most commonly in the form of misgendering and “deadnaming,” being asked unnecessary or invasive questions, and a lack of respect for privacy and confidentiality, which make them feel uncomfortable, anxious, and even unsafe.
It is remarkable that in our study and others, the most-discussed positive experience among TGNB patients is simply being addressed with the correct name and pronouns, a most basic expectation for our cisgender patients. With this said, we were struck by participants’ grace for our system’s shortcomings, their deep appreciation for existing efforts to improve their care, and their consistent emphasis on the importance of listening and responding to feedback. While it is important to identify and amplify positive experiences, it can be more uncomfortable to acknowledge areas for improvement. However, we must remember that we are not alone in this effort. By implementing tangible, sustainable interventions around their recommendations and priorities, we may partner with our TGNB patients in pursuit of the care they deserve: care that is not merely “good enough,” but truly excellent.
Acknowledgments
The authors thank our clinic providers and staff for their support of this project, our participants for their time, candor, and willingness to share their stories and experiences, and the UNC Department of Family Medicine for funding this project.
Appendix 1




Appendix 2
Focus Group Guide

Notes
This article was externally peer reviewed.
Funding: for this project was provided by the Department of Family Medicine at the University of North Carolina at Chapel Hill School of Medicine, through a Family Medicine Innovations Award.
Conflict of interest: The authors have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/37/6/1072.full.
- Received for publication December 3, 2023.
- Revision received February 17, 2024.
- Revision received April 21, 2024.
- Accepted for publication April 29, 2024.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}