Article Text

Abstract
Objective To examine whether genetic testing for smoking-related diseases benefits smoking cessation.
Data sources PubMed, EMBASE, ERIC, PsycINFO, PsychArticles, CiNAHL and socINDEX databases, the search engine Google Scholar, and key-author and reference list searches.
Study selection Randomised controlled smoking cessation interventions using genetic testing for smoking-related diseases.
Data extraction Consistent with the Cochrane guidelines, two reviewers completed the review process (initial n=139) in three phases, title selection (n=56), abstract selection (n=28) and whole paper selection (n=9). From these nine studies, each reviewer extracted information about outcome measures and statistical and methodological quality.
Data synthesis Relevant data were abstracted from included papers and were subsequently subjected to meta-analysis.
Results Interest in genetic testing was relatively high with 60-80% of smokers reporting to be interested. The authors observed positive short-term effects on risk perception, motivation to quit smoking and smoking cessation, but these effects fade at longer follow-ups. Importantly, the authors did not find any evidence of adverse effect of testing negative on the risk-predisposing gene.
Conclusions This systematic review does not provide solid evidence for the proposed beneficial effects of genetic testing for smoking-related diseases on smoking cessation, but does suggest the presence of an immediate motivational effect, such that genetic testing resulted in higher risk perception and more motivation to quit smoking.
- Smoking addiction
- genetic testing
- smoking cessation
- systematic review
- meta-analysis
- cessation
- health services
- smoking caused disease
Statistics from Altmetric.com
- Smoking addiction
- genetic testing
- smoking cessation
- systematic review
- meta-analysis
- cessation
- health services
- smoking caused disease
Introduction
Smoking continues to be the most important behavioural cause of death worldwide.1 2 Although the risks of smoking are well documented and numerous intervention programmes are targeted at smokers, approximately 1.2 billion people still continue to smoke.1 2 About half of all smokers who continue to smoke are estimated to die from a smoking-related disease.1 3 Approximately 1 in 10 deaths is related to a smoking-induced disease and this figure is expected to rise to 1 in 6 by 2030.4
Numerous smoking cessation interventions have been developed in the last few decades, ranging from behavioural interventions to pharmacological treatments.5 However, a large majority of smokers do not fully benefit from current smoking cessation treatments.6 7 For instance, in their systematic review, Silagy and colleagues7 showed that the OR of any nicotine replacement therapy (eg, gum, transdermal patches) versus control was 1.77 (95% CI 1.66 to 1.88). However, only approximately 17% of smokers who received nicotine replacement therapy were abstinent after 12 months or more versus 10% in the control group.7 Although this improvement is considerable, significant and promising, it also indicates that approximately 80% of smokers do not succeed in quitting smoking.
Recent advances in genetic research have created opportunities to use genetic susceptibility information for smoking-related diseases to enhance motivation for smoking cessation. In contrast to simple Mendelian traits, smoking-related diseases mostly represent complex polygenetic associations between genes on the one hand and disease on the other. For instance, where a mutation in the IT15 gene guarantees the development of Huntington's disease,8 the development of smoking-related diseases is caused by an interaction between genetic predisposition and the environment (including behaviour).
The existing literature has identified several genetic variants that put smokers at higher risk for smoking-related diseases, such as lung cancer,9 10 and cardiovascular diseases.11 Genotypes in the L-myc, GSTM1, GSTT1, NQO1 and CYP1A1 genes have all been implicated in elevated disease risks among smokers.12–14 These genes largely interact with smoking behaviour to cause the development of a smoking-related disease while having little to no effect by itself. For instance, people with the LS/SS genotypes in the L-myc gene were found to be highly susceptible to oesophageal and lung cancer, but only when they were exposed to cigarette smoking.13 15
Although the prognostic value of risk factors including genetic risk factors is contested,16 these discoveries do raise the possibility of educating smokers about their genetic susceptibility to such smoking-related diseases to motivate them to quit smoking. Such an approach has also been applied to other common complex diseases, such as Alzheimer's disease17 and familial hypercholesterolaemia.18 Although these studies did not observe beneficial effects of genetic testing on behavioural outcomes concerning adherence to dietary regulations of physical activity guidelines, we still need to establish the value of such an approach for smoking cessation.19
Genetic risk feedback has been argued to enhance motivation for behavioural change more than other types of risk feedback.20 21 That is, risk feedback based on behavioural risks tends to be subject to a process called unrealistic optimism, which states that people often tend to deny their susceptibility to a health problem.22 23 However, genetic risk feedback is arguably not subjected to this process and may therefore result in more accurate perceptions of risk and consequently enhance motivation to quit smoking. Thus, besides examining whether genetic testing for smoking-related diseases results in smoking cessation, it is also worth examining whether the genetic testing affects the proposed cognitive variables underlying their effectiveness, namely risk perception and motivation to quit smoking.
Therefore, the primary purpose of the present review is to examine whether genetic testing for susceptibility to smoking-related diseases is effective in the sense that it results in higher smoking cessation rates in comparison with control groups as well as the proposed cognitive mediators, risk perception and motivation to quit. As a secondary purpose of this review, we also examined whether smokers are interested in and accept genetic testing as a part of a smoking cessation treatment.
Methods
Criteria for considering studies for this review
The general criteria for considering studies in this review concerned the type of study (ie, randomised controlled trials or quasi-randomised controlled trials), the type of participants (smokers 18 years or over), the type of intervention (ie, trails with DNA-based risk feedback, in one arm, against non-DNA-based risk feedback or no risk feedback in the other arm) and the type of outcome (ie, smoking cessation and interest in genetic testing as the primary outcomes and risk perception and motivation to quit smoking as the secondary outcomes). In addition to these criteria, the following inclusion and exclusion criteria were used to determine whether papers were eligible for the review (also see table 1).
Inclusion and exclusion criteria
Search methods for identification of studies
Electronic sources
We searched the PubMed, EMBASE, ERIC, PsycINFO, PsychArticles, CiNAHL and socINDEX databases. Further, we used the search engine Google Scholar to find additional papers on genetic testing and smoking cessation on the internet. The following search term was used: ‘(“smoking” OR “smoking behaviour” OR “smoking behavi*” OR “smoking maintenance” OR “relapse” OR “failed quit attempt”) AND (“biomarker feedback” OR “genetic feedback” OR “genetic risk feedback” OR “genetic susceptibility testing” OR “genetic testing” OR “susceptibility testing” OR “susceptibility feedback”) AND (“abstinence” OR “quit” OR “quit attempt” OR “quit success” OR “cessation” OR “cessation attempt” OR “cessation success” OR “point-abstinence”)’. If available in the databases, we used the standardised subject-related indexing terms of the concepts in the search term. There were no time constraints but we did restrict language to English.
Searching other sources
We performed key-author and reference list searches. In addition, we performed a forward citation search of all potentially eligible studies. There were no time constraints but we did restrict language to English.
Data collection and analysis
Selection of studies
The selection procedure was performed independently by two reviewers. The review process encompassed three phases. Consistent with the Cochrane guidelines,24 we chose to err on the safe side during the selection process. That is, papers that could not be definitively excluded were selected for the following phase in the process. Papers were first reviewed based on their titles only. The abstracts of those papers that were included (and those that could not be definitively excluded based on their title) were then examined in the second phase of the review process. Papers that were thought to be relevant to the review based on their abstracts were included, while those that were judged irrelevant were excluded. In the third and final phase of the selection process, the reviewers examined the entire papers that were included during the previous two phases and relevant data were extracted.
Data extraction and management
All information was abstracted using standardised extraction forms.24 Two authors independently abstracted the relevant information. In case of disagreement, the authors discussed the particular paper until they reached consensus. We abstracted characteristics of the study (ie, country, number of participants), the participants (ie, gender, mean age and number of cigarettes per day) and the genetic testing procedure (ie, the genetic variant tested).
For smoking outcomes, we abstracted abstinence rates. In case multiple abstinence rates were reported (eg, 7 days abstinence, 30 days abstinence and continued abstinence), we extracted the longest-term abstinence rates. We also extracted two important determinants of smoking cessation that genetic testing is argued to affect, namely risk perception and motivation to quit. For interest in genetic testing as part of a smoking cessation treatment, we abstracted smokers' interest in and uptake of genetic testing and again two important determinants of interest and uptake, namely risk perception and motivation to quit.
Assessment of risk of bias in included studies
For the assessment of risk of bias in the included studies, we examined the quality of the study using 22 criteria. Ten questions concerned methodological quality (eg, blinding, sequence generation and other sources of bias), five questions assessed reliability and validity (eg, reliability and validity of primary and secondary assessments) and seven assessed statistical quality of the study (eg, appropriateness of statistical tests conducted, missing data handling, controlling for confounder variables).
Measures of treatment effect
Two main research questions were answered in this review, namely: (1) Does genetic testing of smoking-related diseases result in increased cessation rates among smokers compared with control conditions? and (2) Are smokers interested in undergoing genetic testing for smoking-related diseases with the aim of quitting smoking?
For research question 1, ORs were used as effect sizes; we looked at percentages of smokers who indicated interest in genetic testing for research question 2. Study effects for research question 1 were summarised using forest plots. We used random-effects models to account for the inherent heterogeneity of the studies' different setting, polymorphisms considered and populations. Additionally, we looked at the secondary outcome measures (risk perception and motivation to quit smoking). Effects were described using r. However, as some studies reported risk perception and motivation as dichotomous variables25 26 and others as continuous variables,27 28 we decided not to calculate a pooled estimate for these variables.
Assessment of heterogeneity
We conducted tests of heterogeneity for the studies we included in the meta-analyses using the χ2 test on the I2 statistic.
Assessment of reporting biases
Besides the earlier reported measures of bias in the included studies, we also inspected likely publication bias using funnel plots.
Assessment of subgroup analyses
Besides examining the effects of undergoing genetic testing for smoking-related diseases on smoking cessation, we were also interested in differential effects of the outcome of the testing. That is, we were interested whether testing positive (ie, the predisposing, risk-conferring gene is present) or testing negative (ie, the predisposing, risk-conferring gene is absent) would moderate the effectiveness of genetic testing on smoking cessation. We tested (1) whether having the predisposing gene versus control would result in higher cessation rates, (2) whether not having the predisposing gene versus control would result in adverse effects (ie, result in lower cessation rates) and (3) whether having the predisposing gene versus not having the predisposing gene would also result in higher cessation rates.
Results
Description of studies
We included studies that examined the effect of genetic testing for susceptibility to smoking-related diseases on smoking cessation and studies that examined smokers' interest in genetic testing for smoking-related diseases.
Results of the search
From the initial sample of 136 papers, a total of 25 papers were eligible for extensive review (see figure 1 for the flowchart). Of these, nine papers were included in the review, six concerning the effects of genetic testing on smoking behaviour and three concerning smokers' interest in undergoing genetic testing to establish susceptibility to smoking-related diseases.
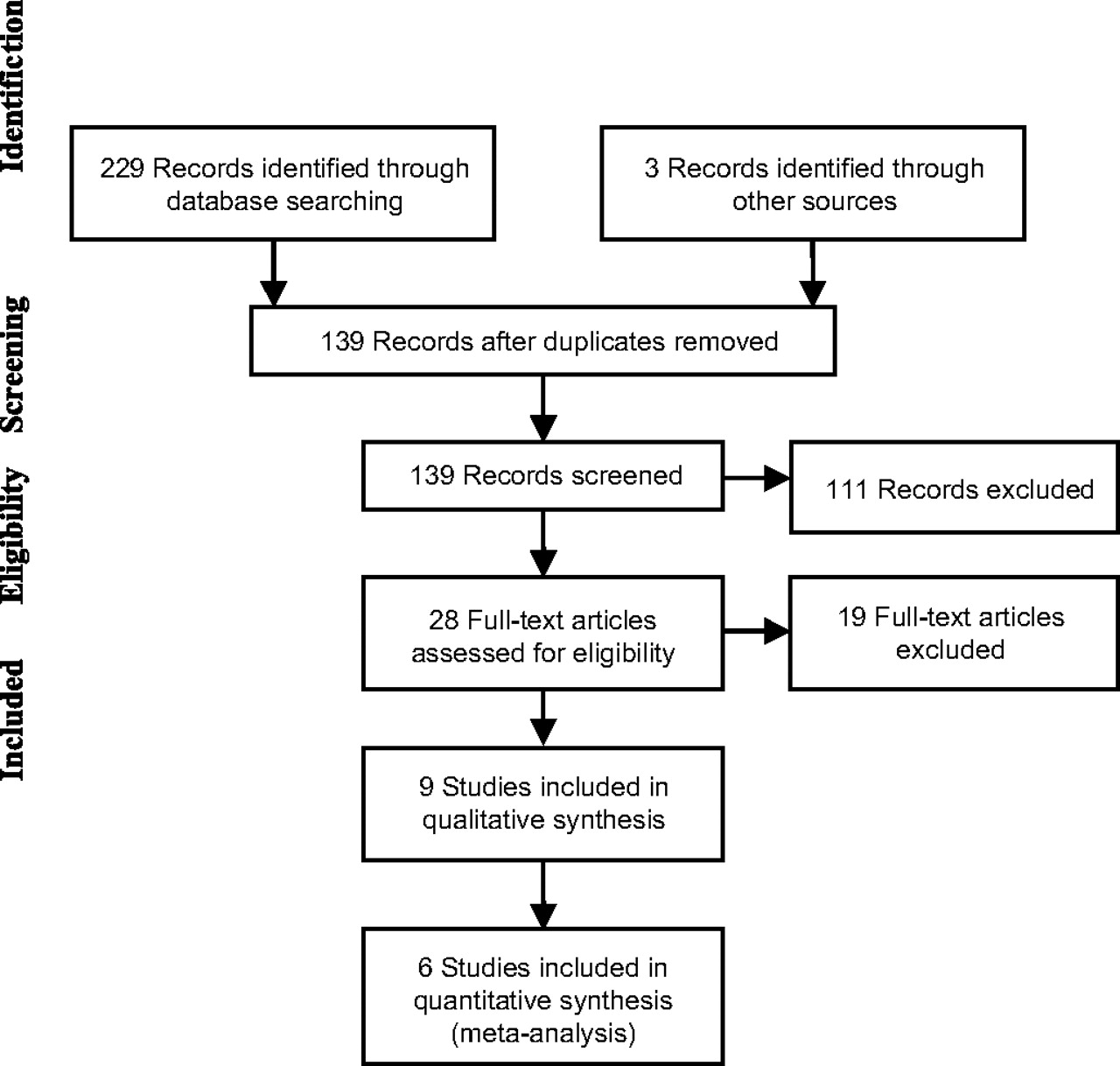
Flowchart of the review process.
Included studies
Table 2 presents an overview of the characteristics of the included studies. Most included studies have been conducted in the USA and Japan, sample sizes ranged from 61 to 697 and mean age varied from 39.2 to 69.0 years. Concerning the effectiveness of genetic testing on smoking cessation, two studies tested smokers for the L-myc gene,25 26 one study tested the CYP2D6 gene29 30 and two studies used the GSTM1 gene.27 28
Characteristics of the studies included in the systematic review
Excluded studies
From the initial sample of 28 papers that were eligible for full review, we excluded 19 studies. Ten studies did not provide smokers with the feedback on the genetic test and were therefore excluded.34–43 Other studies were excluded because they did not assess smoking cessation as an outcome after genetic testing,44 were not randomised controlled trials,45–48 focused on the clinical utility, ethical considerations, etc, of genetic testing for smoking cessation treatments rather than the effectiveness of genetic testing49 or did not present original data.50 51 Finally, one study was retracted after publication and we decided to exclude this study based on this fact.52
Risk of bias
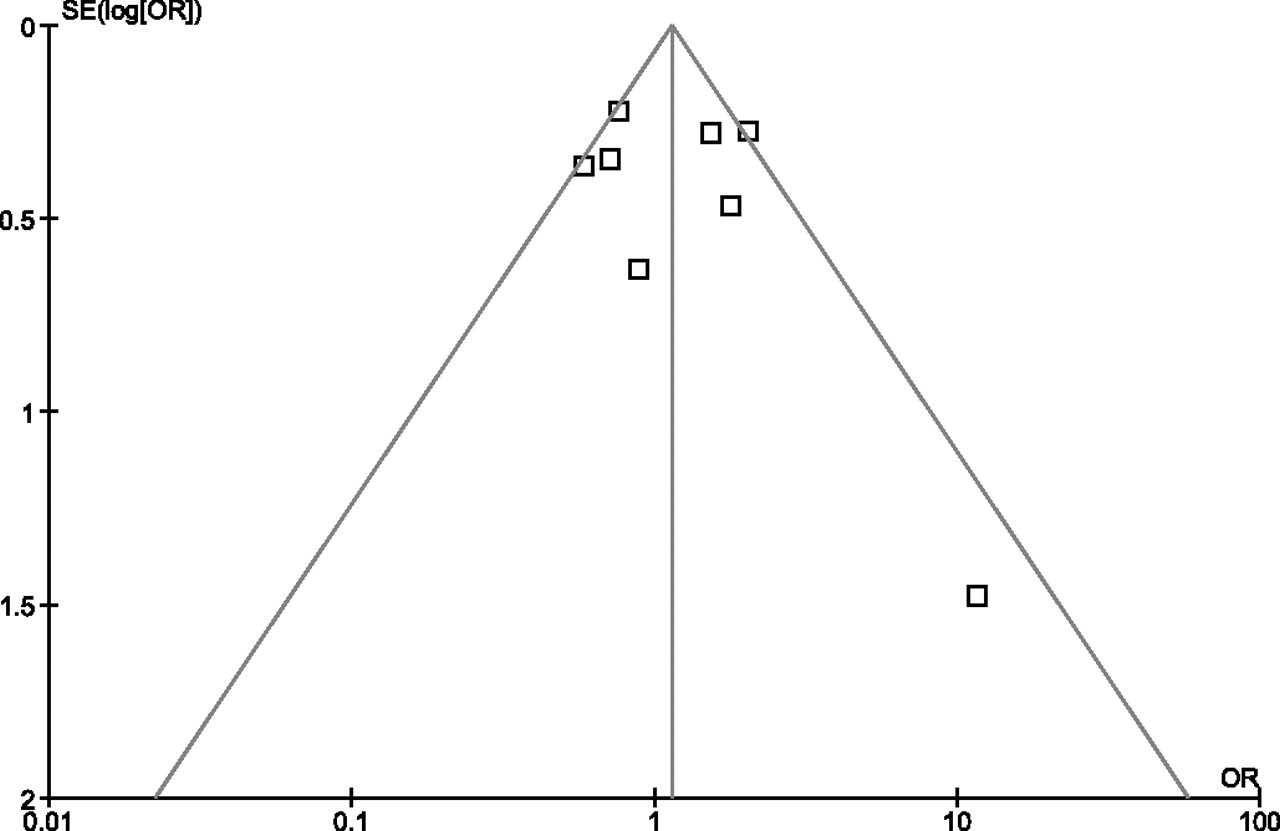
Overall, the studies had fair methodologies (range: 5–8 on a 10-point scale), somewhat questionable statistical quality (range: 2–5 on a 7-point scale), and poor reliability and validity (range: 1–2 on a 5-point scale). Concerning possible publication bias, the funnel plot did not provide any indication of a possible bias (see figure 2).

Funnel plot assessing possible publication bias of studies examining the effectiveness of genetic testing for smoking-related diseases on smoking cessation.
Reported primary outcomes
Smokers' interest in genetic testing
Concerning the interest in genetic testing as part of a comprehensive smoking cessation treatment, we identified three relevant studies (see table 3). Interest in genetic testing is high, approximately 60–80%,31–33 while uptake is considerably lower at approximately 40%.32
Interest in and uptake of genetic testing for smoking-related diseases as part of a smoking cessation treatment and its determinants
Effectiveness of genetic testing
Six papers reporting the results of five studies assessed whether genetic testing versus control enhanced smoking cessation.25–30 In total, these studies included 1694 participants in the genetic testing group and 1316 participants in the control group (see figure 3 for more information on the individual studies). With the exception of one study,27 these studies show no positive effect of being tested for smoking-related diseases on smoking cessation (see table 4). In addition, the pooled estimate of 1.16 (0.77; 1.76) is non-significant (p=0.70).

Forest plot of studies examining the effectiveness of genetic testing for smoking-related diseases versus control on smoking cessation. M-H, Mantel-Haenszel.
Effectiveness of genetic testing for smoking-related diseases on smoking behaviour and proposed working mechanisms
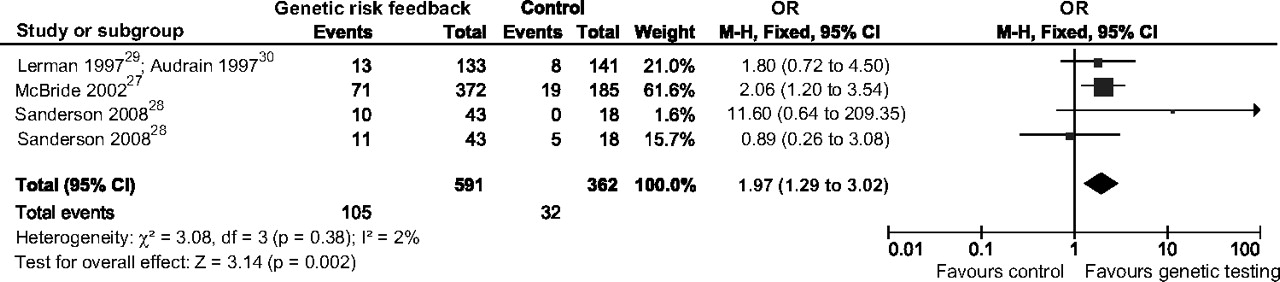
Based on our heterogeneity analyses, we concluded that the studies were fairly heterogeneous (I2=61%, p=0.01) and we decided to distinguish short-term and long-term effects. In the long term (6 months and over), there was no effect of genetic testing on smoking cessation, pooled OR=0.68 (0.57; 1.30), p=0.47. But in the short term (ie, up to 6 months), smokers who underwent genetic testing for smoking-related diseases were significantly more likely to have quit smoking than smokers who had not undergone genetic testing, pooled OR=1.87 (1.20; 2.92), p=0.006 (see figure 4).

Forest plot of studies examining the short-term effectiveness of genetic testing for smoking-related diseases versus control on smoking cessation. M-H, Mantel-Haenszel.
Four papers reporting on four studies reported the differential effects of testing positive (the risk-predisposing genetic variant is present) versus testing negative (the risk-predisposing genetic variant is absent) in comparison with control smokers on smoking cessation.25–28 These studies seemed fairly homogeneous (I2=44%, p=0.11). Overall, smokers who tested positive on the genetic test were marginally more likely to have quit smoking at follow-up than smokers who were not tested, pooled OR=1.53 (0.96; 2.43), p=0.07 (see figure 5). We did not observe any significant difference between positive testers and control smokers at short-term (pooled OR=2.07 (0.85; 5.09), p=0.11) or long-term follow-up (pooled OR=1.34 (0.73; 2.48), p=0.35).
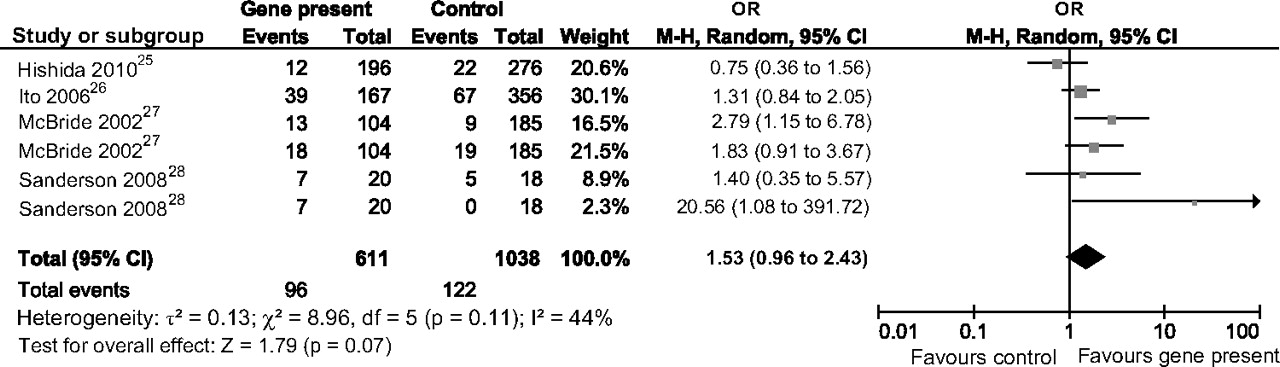
Forest plot of studies examining the effectiveness of testing positive versus control on smoking cessation. M-H, Mantel-Haenszel.
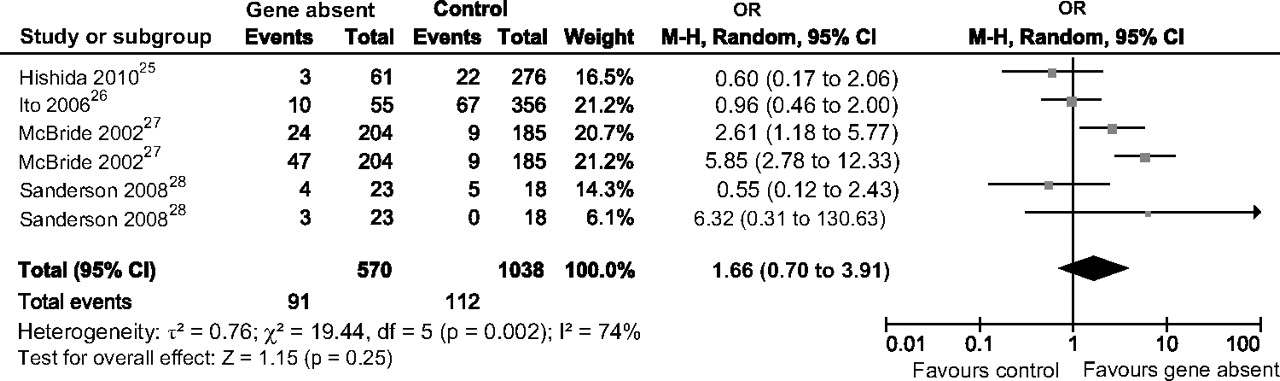
Smokers who tested negative on the genetic test were not less likely to have quit smoking at follow-up compared with smokers who were not tested, pooled OR=1.66 (0.70; 3.91), p=0.25 (see figure 6). Although the studies proved heterogeneous (I2=74%, p=0.002), there were no differences between negative testers and control smokers at short-term (pooled OR=2.54 (0.43; 15.04), p=0.30) or long-term follow-up (pooled OR=1.34 (0.73; 2.48), p=0.35).

Forest plot of studies examining the effectiveness of testing negative versus control on smoking cessation. M-H, Mantel-Haenszel.
Finally, we looked at whether smokers who tested positive for the predisposing genetic variant were more likely to quit smoking than smokers who tested negative. This was not the case, pooled OR=1.15 (0.75; 1.76), p=0.51 (see figure 7). These studies were fairly homogeneous (I2=21%, p=0.28), and accordingly we did not observe any difference between positive testers and negative testers at short-term (pooled OR=1.56 (0.50; 4.85), p=0.44) or long-term follow-up (pooled OR=1.16 (0.71; 1.91), p=0.55).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of studies examining the effectiveness of testing positive versus negative on smoking cessation. M-H, Mantel-Haenszel.
Reported secondary outcomes
Interest in genetic testing
Interest and uptake of genetic testing were found to be positively associated with risk perception and motivation to quit smoking (see table 3). For risk perception, effect sizes of approximately r=0.2531 32 were observed for interest and r=0.12 for uptake.32 Motivation was more strongly related to both interest and uptake of genetic testing for smoking-related diseases, r=0.48 and r=0.22, respectively.32
Effectiveness of genetic testing
Three studies examined the effect of genetic testing on risk perception26 28 29 and four studies examined the effects on motivation to quit.25 26 28 29 In general (see table 4), there seems to be a small immediate effect of genetic testing on risk perception28 29 that disappears at longer follow-ups.26 Similar results were observed for motivation to quit smoking: a small immediate effect28 29 that reduces in size at later follow-ups.25 26
Discussion
Since the end of the 20th century, several studies have been conducted that have investigated the effectiveness of testing smokers for genetic susceptibility to smoking-related diseases on smoking cessation. Interest in genetic testing is relatively high with 60–80% of smokers reporting to be interested. We observed a significant positive effect of undergoing genetic testing on smoking cessation at 6 months follow-up, but this effect was no longer apparent at longer follow-up periods. There were indications that this effect was due to smokers testing positive being marginally more likely to quit smoking than control smokers. Also, and importantly, testing negative for the predisposing gene did not adversely affect smoking cessation. Concerning our secondary outcome measures, we observed a positive short-term effect on risk perception and motivation to quit smoking. Smokers who have undergone genetic testing feel more at risk of developing smoking-related diseases and may be more motivated to quit smoking than controls. Overall, the results suggest that besides achieving a temporary elevation of smokers' motivation to quit smoking and a short-term effect on smoking cessation, genetic testing for susceptibility to smoking-related diseases may not be effective in helping smokers to quit smoking in the long run.
These results raise the question of whether or not to proceed with this line of research in the future. Although this review and meta-analysis is based on only a small number of studies, it does show promise in the sense we did observe a short-term effect on motivation to quit and actual smoking cessation. Future research may investigate how to translate these short-term successes to long-term gains.
In addition, recent research has also focused on the effects of genetic predispositions on smoking addiction and cessation and has pointed towards the possibility of using genetic information to optimise the selection of smoking cessation treatments for individual smokers.53–56 Other research has identified epigenetic changes as a result of smoking. For instance, exposure to cigarette smoking may cause mutation in the CDKN2A gene, which is involved in transforming normal cells to malignant cells.57 58 These two avenues, the genetic basis for smoking behaviour and genetic changes as a result of smoking exposure and how they can be used to promote smoking cessation, warrant further attention.
Based on our review, we formulated several recommendations for future research. First, most studies involved a relatively minimal intervention besides genetic testing. Smoking cessation rates have been found to be relatively low even with more extensive smoking cessation treatments.6 7 From the smoking literature it is obvious that stand-alone programmes are not likely to be successful.7 Instead, the field has moved on to comprehensive quitting programmes that include intensive guidance and follow-up sessions. Close guidance after genetic testing or inclusion of genetic testing procedures in smoking cessation programmes may be needed for successful cessation. Future research should focus on testing the effectiveness of genetic testing for smoking-related diseases as part of a comprehensive smoking cessation treatment rather than as an isolated event.
The second recommendation concerns study design. We recommend using adequate comparative designs in investigating the effectiveness of genetic testing for smoking-related diseases on smoking cessation. For instance, we had to exclude four studies because they did not include a control group. Moreover, in the included studies reported by Hishida et al25 and Ito et al,26 the control condition did not receive any smoking cessation intervention, while the genetic feedback condition was offered additional education besides the biomarker feedback. This difference between conditions makes a direct examination of the effectiveness of genetic testing less reliable. In contrast, the studies by Lerman et al and Audrain et al29 30 compared genetic testing with enhanced usual care. This comparison allows for a better evaluation of the additional effect of genetic testing for smoking-related diseases on smoking cessation.
A third recommendation is to examine possible moderators of the effectiveness of genetic testing as part of a smoking cessation treatment. For instance, while Ito et al26 did not observe an overall effect of genetic testing, smokers without cancer did seem to respond favourably to genetic feedback. Additional moderators that warrant further research may include number of family members who smoke, stage of change59 or level of addiction.60
Fourth, the National Society of Genetic Counselors' Task Force61 proposes that when notifying people about their genetic predispositions, counsellors should (1) interpret family and medical histories to enable risk assessment, (2) educate counselees about issues related to heredity, preventive options (eg, genetic testing) and personal risk and (3) facilitate informed decisions and adaptation to personal risk.62 These tasks have been shown to contribute positively to coping with genetic risks.63 Future research may examine the impact of these three sources of information on the effectiveness of genetic testing for smoking-related diseases on smoking outcomes.
In conclusion, this systematic review and meta-analysis does not provide solid evidence for the proposed beneficial effects of genetic testing for smoking-related diseases on smoking cessation. There are indications of positive short-term effects on risk perception, motivation to quit smoking and smoking cessation, but these effects fade at longer follow-ups. Importantly, we did not find any evidence of adverse effect of testing negative on the risk-predisposing gene. Incorporating genetic testing into a more comprehensive smoking cessation programme with adequate follow-up after feedback of test results may, however, enhance smoking cessation. At the moment, caution is suggested in terms of policies concerning genetic testing for smoking-related diseases as a smoking cessation tool.
Key messages
Genetic testing for smoking-related diseases may produce an immediate motivational effect to quit smoking but does not necessarily have beneficial effects on smoking cessation.
Testing negative for a predisposing gene does not seem to produce adverse effects on smoking cessation.
Close guidance after genetic testing may improve smoking cessation rates.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.