
Abstract
With the lifetime prevalence of shoulder pain approaching 70%, accurate diagnosis and management remains essential. The shoulder is a complex joint with a vast range of motion making it susceptible to injury due to limited bony stabilization. This manuscript shares a simplified, novel approach to evaluating and managing atraumatic shoulder pain based on triaging symptoms on presence or loss of range of motion. In patients with loss of active and passive range of motion, the likely etiologies of pain include adhesive capsulitis or glenohumeral joint arthritis depending on imaging. In patients with preserved active and passive range of motion, implementing specific special testing can help pinpoint the diagnosis, and further guide appropriate management. Ultrasound plays an increasingly key role in diagnosing and managing shoulder pathology.
- Diagnostic Ultrasound
- Physical Examination
- Physical Therapy
- Range of Motion
- Rotator Cuff Injuries
- Shoulder Pain
- Sports Medicine
Introduction
The shoulder is a unique joint that offers extensive range of motion. To achieve this, the shoulder employs soft tissue stabilizers which include the rotator cuff muscles, joint capsule, and ligaments, and has limited bony stabilization which increases function but also increases the risk of injury. Extensive soft tissue stabilization also makes evaluating shoulder pathology a diagnostic challenge. With the lifetime prevalence of shoulder pain approaching 70%,1 primary care clinicians will frequently encounter patients with shoulder pain. The goal of this manuscript is to present a simplified, systematic approach to shoulder pain evaluation and management with a focus on nonacute shoulder pain.
History
Obtaining a detailed history for a painful shoulder is essential for determining the etiology of shoulder pain and initiating the appropriate management. Important factors to elicit in the history are the duration of symptoms and inciting factors including trauma or mechanism of overuse injury.2 Next, it is important to characterize the pain and other associated symptoms such as swelling, stiffness, locking, catching, and/or numbness.3 Determining which motions elicit symptoms can help isolate the anatomy involved in the injury. Inquiring about which activities of daily living, work, sports, or other recreational activities are impacted can help guide the best treatment options for a patient.2,3
Physical Examination
This manuscript will focus on how shoulder special testing can aid in establishing a diagnosis. Special testing will be further discussed and incorporated into the diagnostic algorithm as below and in Figure 1. See Table 1 for special test information including pathology, sensitivity, and specificity. For additional information on performing a physical examination of the shoulder, please reference previously available resources.4,5

Shoulder pain evaluation algorithm.
Shoulder Special Test Sensitivity and Specificity
Terminology
Tendinopathy: general term to describe any pathology of a tendon.6
Tendinitis: acute inflammation of a tendon, usually due to an injury.6
Tendinosis: chronic, degenerative, noninflammatory changes to a tendon.6 The term, tendinosis, is thought to better characterize the underlying pathophysiology associated with chronic tendon pain.
For simplicity, the remainder of this manuscript will describe tendon pathology using the umbrella term, ‘tendinopathy.’
Evaluating Shoulder Pain
This manuscript will focus on a novel, simplified algorithm to evaluate shoulder pain based on whether there is loss of range of motion (Figure 1). Loss of range of motion can be categorized into loss of active and/or passive range of motion.
Preserved Range of Motion
Pain can limit active range of motion during the physical examination which can confound whether range of motion is limited due to pain or mechanical causes. During the physical examination, it can be helpful to coach patients to attempt a full range of motion to provide diagnostic clarity. If a patient cannot complete full range of motion, assessing passive range of motion can provide additional diagnostic information. The following shoulder pain pathologies will typically have preserved range of motion.
Rotator Cuff Tendinopathy/Impingement
History
The rotator cuff muscles include the supraspinatus, infraspinatus, subscapularis, and teres minor. These muscles stabilize the shoulder and injury to the tendons anchoring these muscles can cause significant shoulder pain.7 The patient with rotator cuff tendinopathy will often report referred pain to the lateral shoulder around the mid-deltoid and also may report pain at night.8 Pain is usually worse with overhead activities.8
Key Examination Findings
Evaluate the entire range of motion of the shoulder both passively and actively. Patients typically will have pain with active range of motion but can be coached through a complete active range in abduction, forward flexion, internal rotation, and external rotation. The examiner can consider a diagnostic subacromial lidocaine injection and repeat the examination to delineate true loss of motion versus loss of motion secondary to pain from rotator cuff pathology. The supraspinatus is an important muscle for abduction of the shoulder.9 On examination, patients may have pain with resisted arm abduction or ‘empty can’ testing and may report pain between 60 to 120 degrees of abduction.8 The infraspinatus and teres minor contribute to external rotation and the subscapularis contributes to internal rotation, so pain in these motions may assist with the diagnosis.8,9 Patients are likely to have positive impingement testing as well including pain with passive internal rotation with the elbow flexed in 90 degrees with the shoulder forward flexed at 90 degrees (Hawkins test).5 Pain may also be reproduced with passive internal rotation of the arm and forward flexion (Neer sign).5 These tests result in compression of the rotator cuff tendons and subacromial bursa between the acromion and the humeral head, reproducing pain.
Diagnosis
The diagnosis is typically based on history and physical examination. To augment the examination, there are multiple modalities with which the rotator cuff can be evaluated. Ultrasound (US) and Magnetic Resonance Imaging (MRI) are the best noninvasive studies to visualize tendon injury.10 A radiograph may be obtained to evaluate for bony etiology of shoulder pain and may show signs of rotator cuff tendinopathy with cortical irregularity at the insertion on the humerus or may show calcium deposition within the tendon suggestive of calcific tendinopathy.7 US is commonly the first step in evaluation of the rotator cuff and can visualize tendinopathy and tears clearly.7
Ultrasound
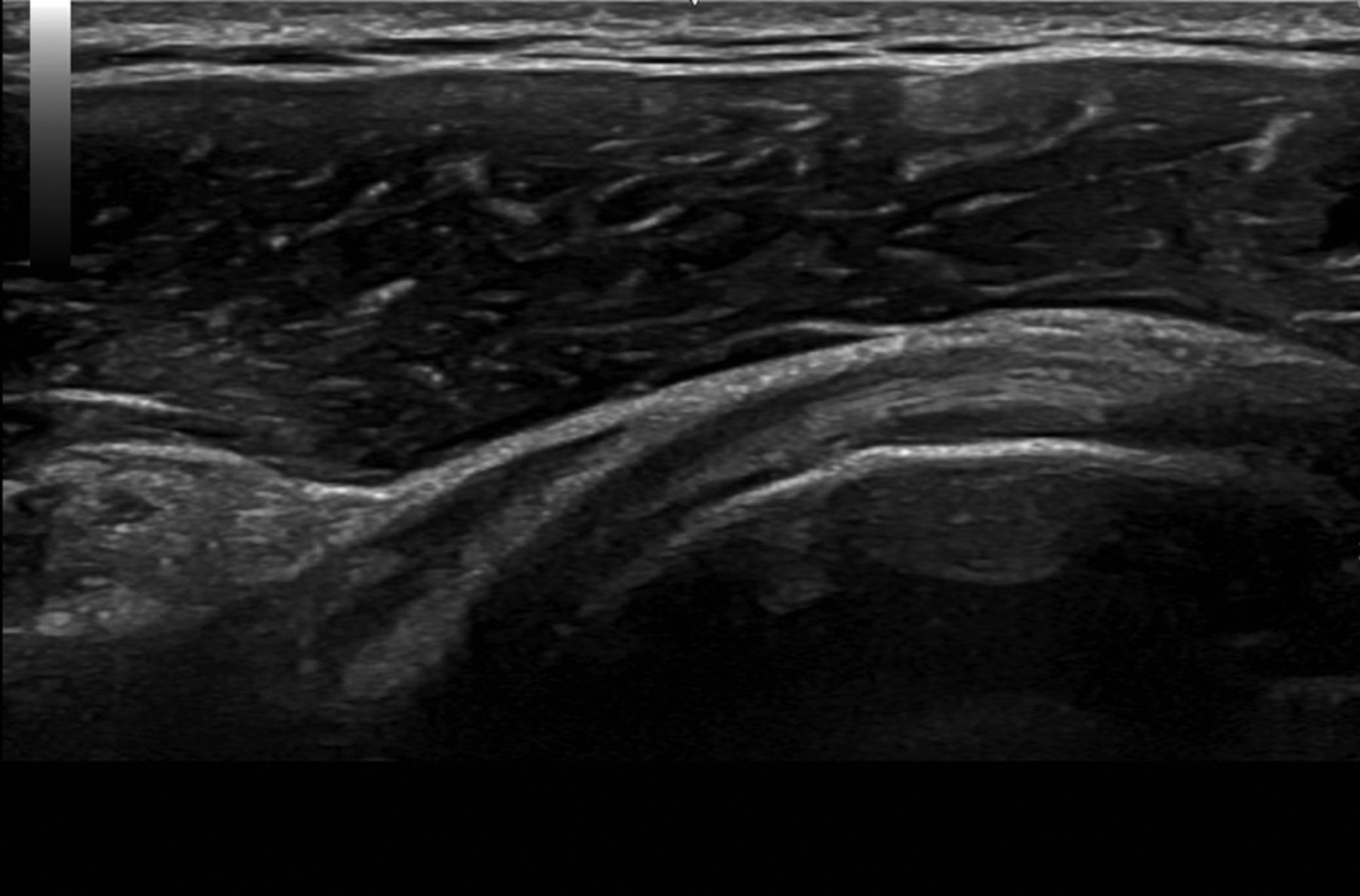
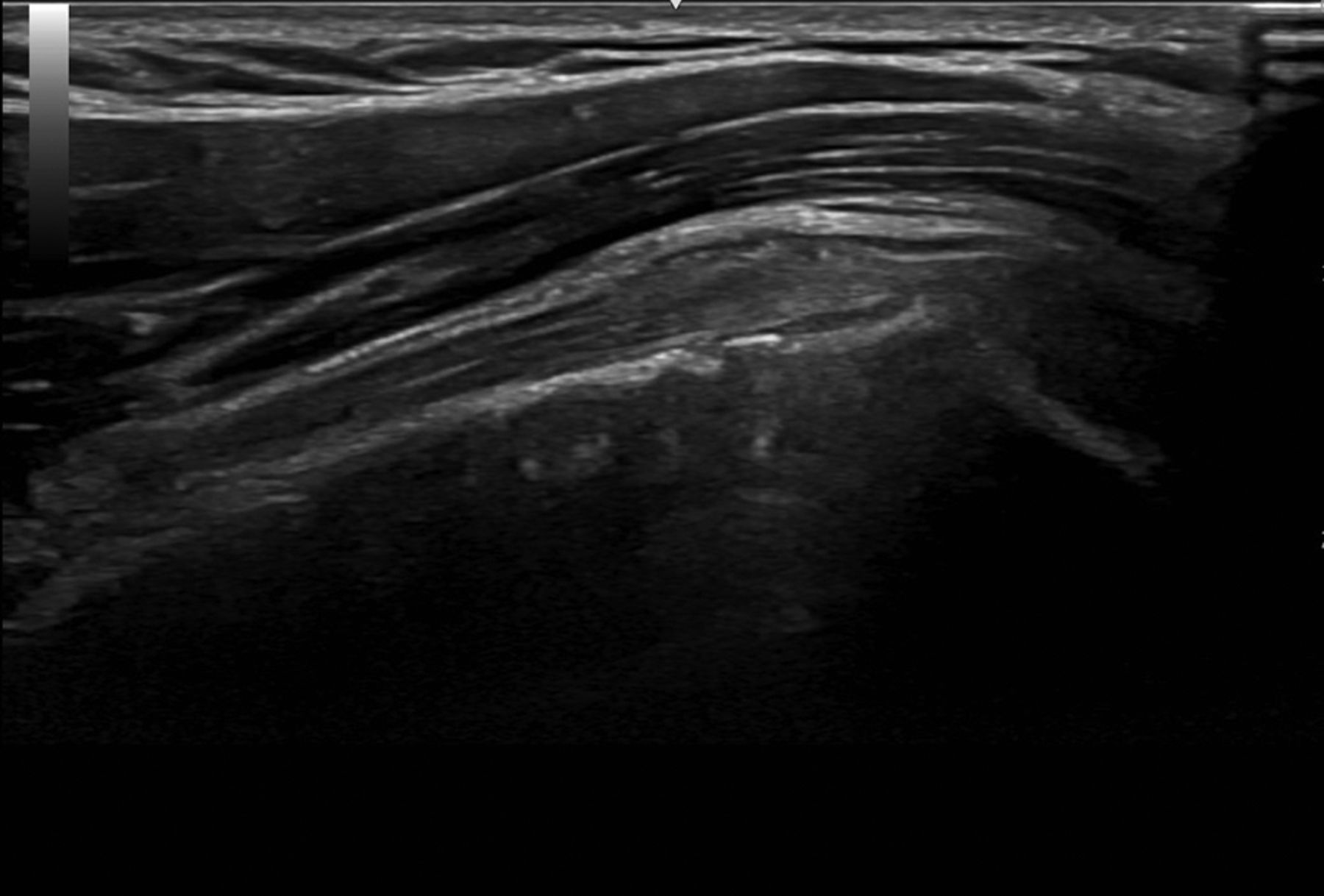
The sensitivity and specificity of US and MRI are nearly equivalent in the evaluation for rotator cuff pathology.7,11 Tendons are hyperechoic (brighter) compared with surrounding tissue with visible fibers that are uninterrupted in longitudinal and sagittal views (Figure 2 to 4).7 When tendinosis is present, the tendon will be hypoechoic (darker) and thickened on US imaging (Figure 5). Calcifications may be seen and will appear in the tendon as small, defined hyperechoic areas.7,12 A tear on US will be seen as a focused area of disruption in the fibers of the tendon (Figure 6).13

Normal supraspinatus tendon

Normal subscapularis tendon.

Normal biceps tendon.

Supraspinatus tendinosis.

Supraspinatus partial tear.
Management
The first step in managing rotator cuff tendinopathy is physical therapy (PT).14 Therapy should be focused on strengthening the individual muscles of the rotator cuff along with the scapular stabilizers.8 Corticosteroid injections into the subacromial space can be used for management of refractory pain, but there is little evidence to show long-term improvement in patients given injections alone compared with injections with concomitant PT.8 Hyaluronic acid injections and platelet rich plasma have limited evidence for their use in the management of rotator cuff disease, although more research is being done on their efficacy.15 US guided needle fenestration or percutaneous tenotomy is another emerging treatment option.16 Surgical referral can be considered for persistent pain with rotator cuff tendinopathy that has failed conservative treatment.8 Small tears can be debrided while higher grade partial tears or full thickness tears may benefit from repair.7
Biceps Tendinopathy
History
It can be difficult to diagnose biceps tendinopathy due to its overlap with many other causes of shoulder pain. Patients will often report anterior shoulder pain that may radiate down the biceps. The pain will be aggravated by overhead movements including forward flexion,2 especially in overhead athletes or individuals with repetitive overhead work.17 Patients with instability of the tendon may experience clicking or popping and may even hear a snapping sound with overhead motions.2,3
Key Examination Findings
A key finding on examination is pain to palpation over the bicipital groove.2,18 With biceps tendinopathy, patients may have pain with resisted forward flexion of the arm with the palm up (Speed’s test).5 They may also have pain with resisted supination with the elbow flexed at 90 degrees (Yergason’s test).4 These tests are sensitive but not specific to biceps pathology as these tests can also reproduce pain when rotator cuff pathology is present.3,19 In the case of rupture of the proximal biceps tendon, the examiner may see a bulge in the upper arm due to biceps muscle contraction, particularly with elbow flexion.2
Diagnosis
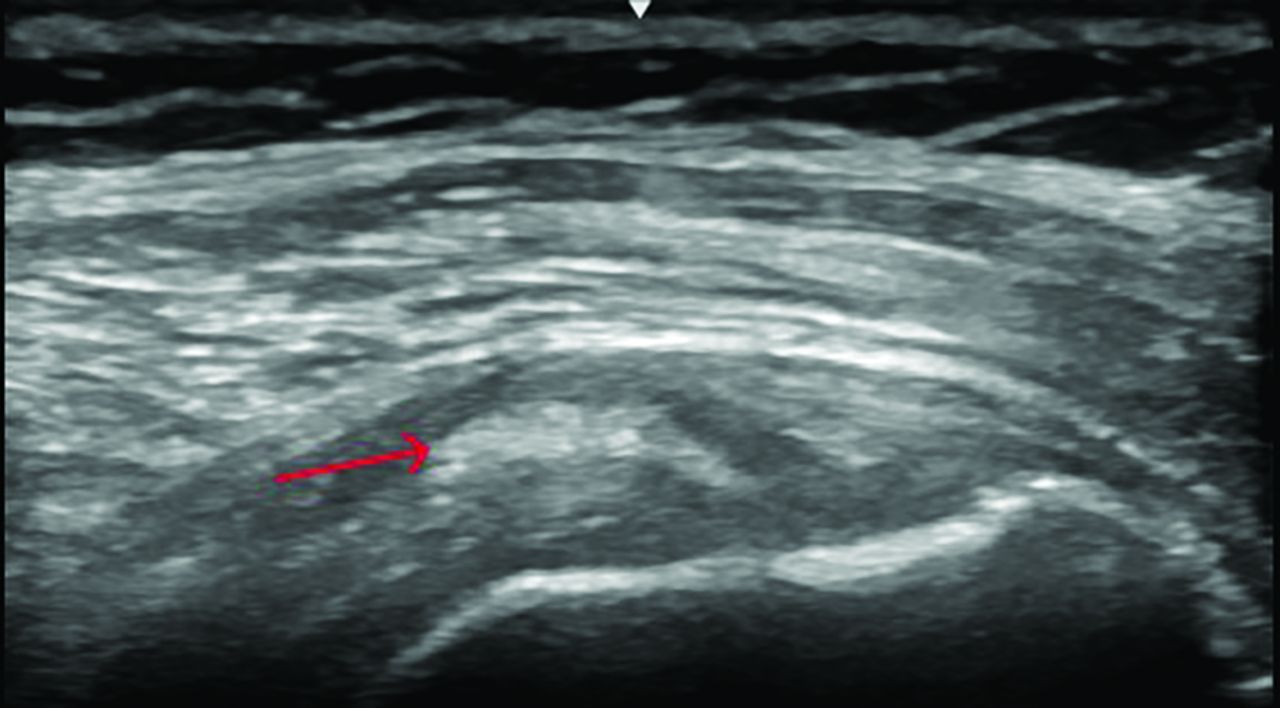
The diagnosis is primarily clinical, based on history and physical examination. MRI and ultrasound can aid in the diagnosis of biceps tendinopathy if the etiology remains unclear.2,20,21 Biceps tendinopathy is seen on ultrasound as tendon thickening with heterogenous hypoechoic changes(Figure 7).22 There may be edema surrounding the tendon on ultrasound in cases of acute tendinitis. A radiograph may be helpful to rule out other causes of shoulder pain but will not visualize the biceps tendon.3

Biceps tendinosis.
Management
Biceps tendinopathy is often associated with rotator cuff pathology. Identifying and treating rotator cuff pathology, if present, is important in the treatment of biceps tendinopathy.17 Management begins with conservative measures including rest, over the counter pain management, and physical therapy.2,3 Rehabilitation programs should focus on stabilization of the shoulder through strengthening the rotator cuff, deltoid, and scapular muscles.17 Activity modification until resolution of pain with gradual return to activity can prevent reinjury.3,17 Corticosteroid injections can be performed for pain relief if symptoms are not improving with PT. The injection is typically done under ultrasound guidance into the tendon sheath to avoid injection into the tendon which can increase the risk of tendon rupture.2,3,17,23 If there is no improvement with these measures, surgical intervention including biceps tenotomy or tenodesis can be considered.2,3
Acromioclavicular (AC) Joint Pathology
History
AC joint pathology presents as pain over superior aspect of the shoulder, lateralizing over the AC joint. Risk factors including repetitive cross body loading including weightlifting, repetitive work, or history of injury/trauma including AC separation.
Key Examination Findings
The most common examination finding is tenderness to palpation directly over the AC joint.24 Patients may have pain reproduced with passive crossbody adduction of the arm with the shoulder in 90 degrees of flexion (crossbody adduction test).5 The crossbody adduction test, also known as the scarf test, has the highest sensitivity for AC joint pathology.24
Diagnosis
In addition to the physical examination, a Zanca view shoulder radiograph can further evaluate the AC joint for arthritis, separation, or fracture.24 Ultrasound evaluation can identify if AC joint effusion is present.24 Ultrasound can also evaluate for tenderness with sonopalpation. In addition, US can be used for diagnostic and therapeutic AC joint injection for further diagnostic clarity and pain management.25 The utility of MRI is limited for AC joint pathology.24
Management and Prognosis
AC joint pathology management depends on the diagnosis. AC joint arthritis is managed similar to glenohumeral joint arthritis with rehabilitation, corticosteroid injections, or surgical management with distal clavicle resection.26 Avoiding crossbody maneuvers can help manage pain during acute flares. Management of AC sprains varies from conservative management with a short course of immobilization to surgical ligamentous repair depending on grade of injury.26
Labral Pathology
History
Patients with anterior labral pathology will typically present with anterior shoulder pain around the bicipital groove.27 Patients at risk for labral pathology, specifically superior labrum anterior posterior (SLAP) lesions, include overhead athletes and those who perform heavy manual labor.28 Individuals may also present with mechanical symptoms including clicking, particularly when their arm is abducted and externally rotated.29 Posterior labral tears are most commonly caused by direct shoulder injury by falling on an outstretched hand.27
Key Examination Findings
In addition to the basic shoulder examination, a combination of special tests is recommended as there is not a single test proven to have high sensitivity and specificity for labral pathology. These tests include anterior glide test, compression rotation test, active compression (O’Brien’s) test, and crank test.30,31
Diagnosis
The diagnosis of labral pathology is based on history, examination, and imaging.32 MR Arthrogram is more sensitive in diagnosing labral pathology than the conventional shoulder MRI.32 Radiograph and ultrasound will not evaluate the anterior glenoid labrum but can be considered to rule out other concurrent shoulder injury.33 Arthroscopy is the gold-standard for diagnosing labral tears.33
Management and Prognosis
Management depends on patient’s symptoms, age, and functional requirements. Many overhead athletes will have asymptomatic SLAP tears and do not need additional treatment or intervention.34,35 It is sometimes thought to be a normal, adaptive response for higher level athletes.35 In addition, SLAP lesions can be present in up to 70% of asymptomatic middle-aged patients.36 Thus, the management can be confounded as this may be an incidental finding on MRI and not the primary source of pain. A careful shoulder examination to pinpoint the etiology and location of pain is the most informative in determining if the source of pain is the labrum. First line treatment for symptomatic anterior labral tears includes a focused physical therapy program. If no improvement, surgical evaluation is indicated as management varies based on the type of tear, which remains outside of the scope of this manuscript. Anterior labral tears which occur from trauma or shoulder dislocation should be referred for surgical evaluation.37
Loss of Active and Passive Range of Motion
Adhesive Capsulitis
History
Incidence is approximately 3 to 5% of the population and up to 20% in those with diabetes.38 Pain typically starts at night and presents as vague, generalized shoulder pain. Many patients will endorse referred pain to the mid deltoid region over the lateral aspect of the upper arm.39 Pain precedes the loss of range of motion and external rotation tends to be the first motion lost, followed by global loss of motion.39 Comorbid conditions associated with adhesive capsulitis include hypothyroidism and diabetes.38
Key Examination Findings
Loss of active and passive range of motion is a hallmark of adhesive capsulitis. Individuals tend to have overlapping special test findings including pain with impingement maneuvers (Neer and Hawkins test), biceps provocative maneuvers, and pain with active and passive shoulder range of motion.
Diagnosis
History, examination, and imaging can aid in the diagnosis of adhesive capsulitis. In patients with loss of active and passive range of motion, a radiograph can help rule out glenohumeral joint osteoarthritis, which can also result in loss of passive range of motion. If radiography does not show significant arthritis, adhesive capsulitis is the most likely diagnosis in the setting of loss of passive range of motion. There are secondary imaging findings that can suggest adhesive capsulitis on diagnostic ultrasound and MRI including joint capsule thickening and coracohumeral ligament thickening.40 These are nonspecific findings and advanced imaging is not necessary for further workup if the history and examination is consistent.
Management
Initial management includes physical therapy and over the counter medications for pain management. If pain is severe and limiting activities of daily living including sleep, injection options can be considered including US guided glenohumeral joint injection.41 Another injection option for management is US guided hydrodilation which entails injecting high volume fluid such as sterile water or sterile saline in addition to a local anesthetic and a steroid with the intent to dilate the joint capsule.42 Finally, surgical management can be considered including manipulation under anesthesia or capsular release. While these options may help with pain management, they have not been proven to consistently shorten the time course of this disease.43 Adhesive capsulitis is thought to be self-limited with a typical duration of 12 to 36 months, however, some individuals can have long-term sequelae.44
Glenohumeral Joint Osteoarthritis
History
Individuals with glenohumeral joint arthritis may endorse insidious, deep, anterior shoulder and upper arm pain with associated stiffness and progressive loss of range of motion. Risk factors include history of instability, rotator cuff pathology, history of trauma, genetics, and obesity.45
Key Examination Findings
On examination, there may be tenderness to palpation over the anterior joint line. In later stage disease, patients may lose active and passive range of motion, particularly with external rotation and abduction.46 Special testing for biceps tendinopathy, rotator cuff tendinopathy and labral pathology may be positive and may confound evaluation.
Diagnosis
Shoulder radiographs, including Grashey view or axillary view, is the recommended imaging to evaluate for glenohumeral joint arthritis.47 Reduction in joint space with subchondral sclerosis and osteophyte formation is characteristic of glenohumeral joint arthritis (Figure 8).47 In patients with multiple positive special tests, loss of active and passive range of motion, and radiograph findings of arthritis, the likely diagnosis is glenohumeral joint arthritis.

Glenohumeral joint osteoarthritis.
Management and Prognosis
A strengthening and stretching program focusing on shoulder joint capsule, deltoid, rotator cuff, and scapular stabilizers is a key component of rehabilitation.48 If pain persists, injection options include US guided corticosteroid injection into the glenohumeral joint or suprascapular nerve block can be considered for pain management.48,49 It is important to note, injection options will not necessarily improve the patient’s range of motion but can decrease pain and increase function. Finally, surgical options can be considered if no improvement with conservative management including arthroscopic management or shoulder arthroplasty including reverse total shoulder arthroplasty or total shoulder arthroplasty.48
Loss of Active Range of Motion, Preserved Passive Range of Motion
Rotator Cuff Tear
History
There is overlap in symptoms of rotator cuff tendinopathy and rotator cuff tear. Both present with pain with abduction and external rotation of the arm. Individuals with a rotator cuff tear may have a history of trauma such as a fall on an outstretched hand or a direct fall on the shoulder.
Key Examination Findings
Key examination findings include weakness in the motion of the affected muscle. Patients with a supraspinatus tear will present with weakness with abduction. Infraspinatus injury may present with weakness with external rotation and subscapularis tears present with weakness with internal rotation or difficulty with push-off test.50
Diagnosis
The diagnosis can be made clinically with evidence of weakness on examination. However, pain secondary to partial tears or tendinopathy can also contribute to weakness and difficulty assessing strength, so obtaining advanced imaging is often necessary to confirm the diagnosis. Radiographs are helpful to evaluate for cortical irregularities of the humerus, a high riding humerus, or rotator cuff arthropathy which can be present in the setting of chronic, complete rotator cuff tears (Figure 9).50 Ultrasound and MRI as reviewed above are the most helpful imaging modalities for evaluating for rotator cuff tears.

Rotator cuff arthropathy.
Management and Prognosis
Management depends on time course and nature of injury. In an acute, traumatic, full-thickness rotator cuff tear, the standard of care particularly in young, active patients is early rotator cuff repair with a goal of repairing within 3 to 4 months from injury.50,51 Patients with an atraumatic tear or partial tear can start with nonoperative management similar to rotator cuff tendinopathy as described above with physical therapy, injection options for pain management, and consider surgical management if no improvement with nonoperative options.14,50
Less Common Causes of Shoulder Pain
Thoracic Outlet Syndrome
Neurogenic, arterial, and venous thoracic outlet syndrome is caused by trauma, repetitive motion, and variations in anatomy around the first rib.52 Close to 90% with neurogenic thoracic outlet syndrome present with shoulder pain, so maintaining a broad differential can aid in diagnosis.53 Multiple special tests can be used during examination including Adson’s test, elevated arm stress test, and upper limb tension tests. These test are not sensitive nor specific and may lead to false positives.54 Vascular imaging to rule out deep vein thrombosis and doppler to evaluate arterial flow are the best initial tests when evaluating for thoracic outlet syndrome.55 Evaluation by vascular surgery is recommended if there is suspicion for thoracic outlet syndrome.
Brachial Neuritis
Brachial Neuritis, also known as Parsonage-Turner Syndrome, presents as sudden onset, severe pain without significant trauma or injury.56 Pain is typically worse at night. The next stage of the condition entails resolution of pain but progressive shoulder weakness.57 Diagnosis is made clinically and by evaluating nerve conduction with an EMG along with MRI of the brachial plexus. This is a self-limiting condition with around 90% recovery within 3 years.58 It may be reasonable to use oral steroids in the acute phase for pain management, but this has not been shown to change the time course of the disease.57
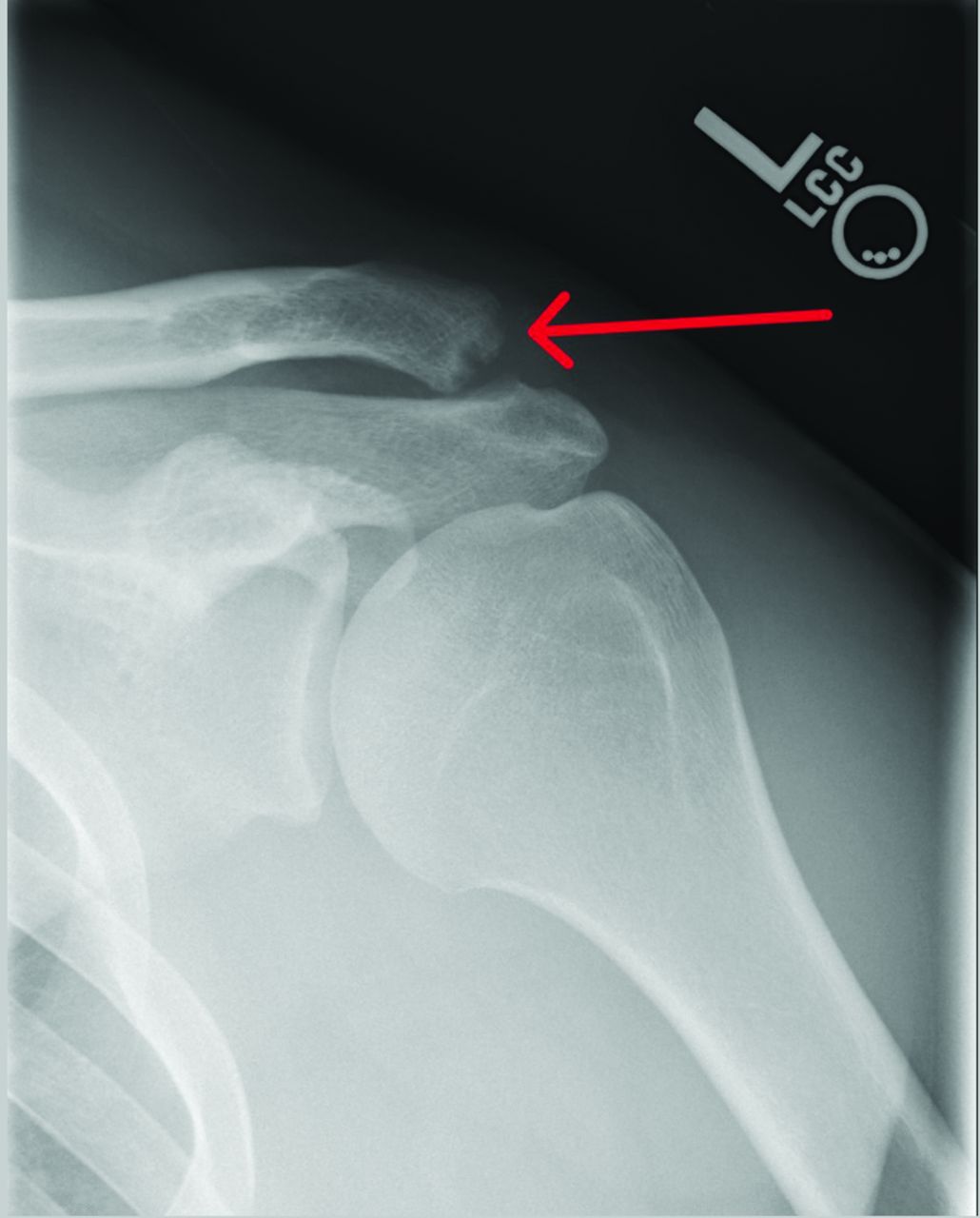
Distal Clavicle Osteolysis
Distal clavicle osteolysis may develop in individuals who weightlift or perform repetitive heavy lifting at work.59 This results in a ‘moth eaten’ appearance of the distal clavicle due to repetitive bony stress from microfractures and repair attempts (Figure 10).60 Examination is significant for pain over the AC joint and pain with AC provocative maneuvers as described above. Treatment includes activity reduction/modification and consideration of corticosteroid injections for symptom management. Severe cases are managed with distal clavicle resection.59

Distal clavicle osteolysis.
Non-Musculoskeletal Causes of Shoulder Pain
While the focus of this review is on musculoskeletal etiology of shoulder pain, clinicians should maintain a broad differential to evaluate and workup for nonmusculoskeletal etiology of shoulder pain including referred cardiac, thoracic, spinal, or abdominal pain.
Conclusion
The shoulder is a complex and unique joint which can be diagnostically challenging. Triaging shoulder pain based on presence or loss of range of motion and special tests can guide the differential and lead to more accurate diagnosis and management of shoulder pathology.
Notes
This article was externally peer reviewed.
Conflict of interest: The authors have no conflicts of interest to report.
Funding: There were no sources of funding for this project.
To see this article online, please go to: http://jabfm.org/content/37/6/1156.full.
- Received for publication March 11, 2024.
- Revision received May 8, 2024.
- Revision received June 4, 2024.
- Accepted for publication June 10, 2024.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- History
- Physical Examination
- Terminology
- Evaluating Shoulder Pain
- Preserved Range of Motion
- Loss of Active and Passive Range of Motion
- Loss of Active Range of Motion, Preserved Passive Range of Motion
- Less Common Causes of Shoulder Pain
- Non-Musculoskeletal Causes of Shoulder Pain
- Conclusion
- Notes
- References
- Figures & Data
- References
- Info & Metrics