
Abstract
Background: Identifying and addressing social needs is important to improve health for older adults with type 2 diabetes mellitus (T2DM). However, few studies have examined the association between social needs and T2DM-related outcomes among older populations within integrated health care systems. This study examined the association between social needs and DM-related outcomes among older adults with T2DM receiving care at Kaiser Permanente Northwest.
Methods: From a cohort of 1954 Medicare members ages 65 and older who completed a social needs questionnaire, we examined the association between 5 dichotomous (yes vs no) social needs measures (financial strain, food insecurity, housing instability, social isolation, and transportation needs) and 3 DM-specific outcomes in the 12 months after assessment: 1) good glycemic control (HbA1c < 8%); 2) any DM-specific emergency department (ED) utilization; and 3) any DM-specific hospital admissions.
Results: About 40% of the study population reported 1 or more social needs. Financial strain (OR = 0.56, 95% CI = 0.36-0.85), food insecurity (OR = 0.47, 95% CI = 0.28-0.81) and housing instability (OR = 0.50, 95% CI = 0.25-0.99) were associated with lower odds of good glycemic control. All 5 social needs were associated with higher ED utilization (financial strain: OR = 1.65, 95% CI = 1.17-2.33; food insecurity: OR = 1.62, 95% CI = 1.02-2.57; housing instability: OR = 2.14, 95% CI = 1.23-3.75; social isolation: OR = 1.36, 95% CI = 1.06-1.74; transportation needs: OR = 1.83, 95% CI = 1.23-2.71). Financial strain was also associated with higher hospital admissions (OR = 1.77, 95% CI = 1.17-2.68).
Discussion: Associations between social needs and DM-specific outcomes demonstrate the need to develop programs to address social needs in the clinical setting and test whether such interventions improve DM-related outcomes.
- Financial Stress
- Food Insecurity
- Housing Instability
- Integrated Health Care Systems
- Medicare
- Social Determinants of Health
- Social Isolation
- Surveys and Questionnaires
- Type 2 Diabetes Mellitus
Background
Examining social needs among older adults with type 2 diabetes mellitus (T2DM) in the United States is an important research area, as nearly 30% of adults ages 65 and older have T2DM,1 resulting in over $400 billion in health care costs annually2 and older adults experience high levels of social needs. About 25% report social isolation and loneliness,3 nearly 1 in 10 experience food insecurity,4 and 5 to 7% experience financial strain.5
Further demonstrating the importance of studying social needs within the T2DM population, previous research found that social needs are associated with negative health and health care utilization outcomes among adults with T2DM. Specifically, food insecurity, financial strain, housing, and transportation needs are associated with suboptimal DM-related outcomes, including lower medication adherence6 and poor glycemic control.7⇓–9 Moreover, the presence of social needs may lead to delayed or forgone needed medical care, as well as increased emergency department and inpatient visits.9⇓⇓⇓⇓–14
Although some studies have examined the association between social needs and T2DM-related outcomes for older adults,13–15 few have been conducted in large, integrated health care systems. Studying these associations in large, integrated health care systems among older populations can both: 1) provide insights from systems with comprehensive clinical, demographic, social need, and health care utilization data and 2) help to target quality improvement interventions to those with specific social needs. With this background in mind, the primary objective of this study is to examine the association between social needs and DM-related outcomes among a population of Medicare patients receiving care in a large integrated health care system.
Methods
Study Design
This was an observational cohort study of 1954 Medicare Advantage enrollees (ages 65 years or older) who were members of Kaiser Permanente Northwest (KPNW), an integrated health system that provides care for patients who reside in Oregon and southwest Washington.
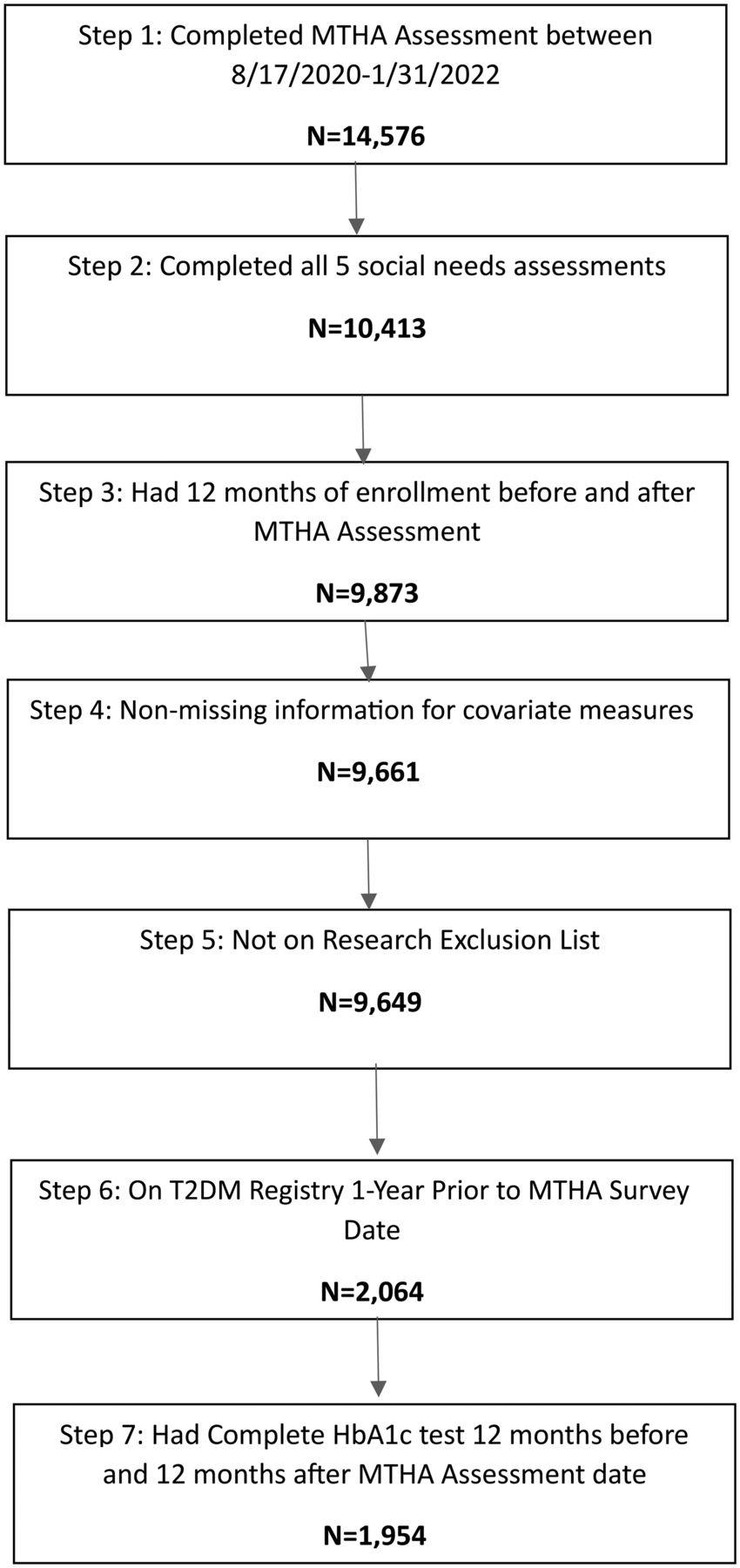
Patients were part of a larger study16 that included the following enrollment criteria: 1) completion of a Medicare Total Health Assessment (MTHA) survey during usual care between 8/18/2020 and 1/31/2022 (index date is defined as date of survey completion); 2) completion of all 5 social needs assessments on the MTHA survey: financial strain, food insecurity, housing instability, social isolation, and transportation needs; 3) health plan enrollment for 12 months before and after their index date; 4) no missing covariate data; 5) not on the KPNW research exclusion list; 6) on the KPNW T2DM registry for 12 months before their index date and 12 months after their index date; and 7) completion of an HbA1c test within 12 months before and 12 months after their index date. A process flow of this enrollment criteria is described in Figure 1. The MTHA16⇓–18 and KPNW T2DM Registry have been described previously.19 A recent study analyzed similar social needs and all-cause utilization outcomes for the full older adult population using the MTHA survey.16

Population process flow. Abbreviation: MTHA, Medicare Total Health Assessment.
Survey data from the MTHA, as well as clinical and health care utilization outcome measures from the electronic health record (EHR), are housed in the Research Data Warehouse (RDW) at the Kaiser Permanente Center for Health Research (CHR), which has been described previously.20 This study was approved by the KPNW Institutional Review Board.
Measures
Outcome Measures
Three outcome measures were assessed in the 12 months after the index date: 1) good glycemic control, defined as HbA1c < 8%; 2) DM-specific emergency department (ED) visits and 3) DM-specific hospital admissions. Although previous research has used a HbA1c cutoff <7%,19 we selected less restrictive of HbA1c < 8%, given guidelines suggest a less rigorous HbA1c cutoff is more appropriate in older adults.21 If multiple HbA1c tests were conducted in the 12 months after the index date, the first HbA1c test was selected. DM-specific utilization outcomes were based on E10**-E11** ICD-10 codes as encounter diagnoses for ED visits and hospital admissions.
Independent Variables
The primary independent variables were the presence of 5 social needs (financial strain, food insecurity, housing instability, social isolation, and transportation needs) measured as binary (yes/no) measures, assessed during the index MTHA survey. A description of these social needs is provided in Table 1.
Description of Social Needs Measures.
Covariate Measures
Covariate measures for the analysis were identified from either the MTHA survey or the EHR. Measures identified from the MTHA survey included: highest education level completed, self-reported overall health, and self-reported mental health. Measures identified from the EHR included: neighborhood deprivation index (NDI)22; age, sex, race, ethnicity, Charlson Comorbidity Index (CCI),23,24 HbA1c status in the 12 months before index date, and DM-specific ED utilization and hospital admissions in the 12 months before index date. If multiple HbA1c tests were conducted in the 12 months before the index date, the first HbA1c test was selected.
Analysis
First, descriptive analyses were conducted for the study population. Next, collinearity diagnostics were used to assess collinearity among each of the social needs variables and the covariate measures. Because no collinearity was found, all covariate measures were included in final logistic regression models. Five logistic regression models were constructed for each dichotomous outcome measure, with each social need variable analyzed as a dichotomous measure (yes vs no [ref. group]).
Results
Sample Characteristics (Table 2). About 60% of the study population were between ages 65 and 74, 52% were male, and nearly 90% were White and non-Hispanic. Nearly 35% reported having a college degree or higher level of education, and on average, patients lived in neighborhoods that had low levels of neighborhood deprivation (mean NDI score = -0.2 ± 0.6). About 30% of the population reported their overall health as “fair” or “poor”; over 60% had a CCI score of 2 or higher. About 20% and 10%, respectively, had any DM-specific ED utilization and DM-specific hospital admissions in the 12 months before the MTHA survey.
Population Characteristics
Type and Number of Social Needs (Table 3). Forty percent of respondents identified at least 1 social need on the MTHA; 3.5% reported 3 or more needs. The most reported social need was social isolation (31.0%), followed by financial strain (9.6%), transportation needs (6.7%), food insecurity (4.9%) and housing instability (3.1%).
Description of Social Needs and Outcome Measures in Population
Logistic Regression Results (Table 4)
Logistic Regression Results: Association Between Individual Social Needs and DM-Specific Outcomes
Association Between Social Needs and HbA1c Control
Presence of financial strain (OR = 0.56, 95% CI = 0.36–0.85), food insecurity (OR = 0.47, 95% CI = 0.28–0.81), and housing instability (OR = 0.50, 95% CI = 0.25–0.99) were associated with lower odds of having good glycemic control. No other social needs measures were associated with glycemic control as measured by HbA1c values.
Association Between Social Needs and Diabetes-Specific ED Utilization and Hospital Admissions
The presence of each of the 5 social needs was associated with higher ED utilization in the 12 months following the index date: financial strain (OR = 1.65, 95% CI = 1.17–2.33), food insecurity (OR = 1.62, 95% CI = 1.02–2.57), housing instability (OR = 2.14, 95% CI = 1.23–3.75), social isolation (OR = 1.36, 95% CI = 1.06–1.74) and transportation needs (OR = 1.83, 95% CI = 1.23–2.71). The presence of financial strain was associated with higher hospital admissions in the 12 months following the index date (OR = 1.77, 95% CI = 1.17–2.68).
Discussion
We found nearly 4 in 10 adults ages 65 and older with T2DM reported at least 1 unmet social need, with over 10% reporting 2 or more needs. Financial strain, food insecurity, and housing instability were associated with poor glycemic control, and all 5 social needs were associated with DM-related ED utilization in the year following assessment. Finally, financial strain was associated with DM-related hospital admissions in the year following assessment.
Our study results complement previous research examining social needs and health outcomes among older people with diabetes. As in our study, Ryan et al. (2023)13 found that loneliness and transportation needs were associated with higher ED utilization. In addition consistent with our findings, Massey et al. (2023)25 found that food insecurity was associated with poorer glycemic control, while Walker et al. (2021)26 found that increased financial strain was associated with worse glycemic control. While previous research found that lack of housing was associated with poorer glycemic control in a veteran population27 our study seems to be one of the first to find an association between housing instability and worse glycemic control in a Medicare population.
Our finding that food insecurity was associated with increased ED utilization is similar to other research findings in the published literature. Although not DM-specific,28 Estrella and colleagues (2021) found that those with food insecurity were more likely to be frequent users of the ED. While the exact causal mechanisms are unclear, food insecurity among those with T2DM may lead to poor disease management, leading to complications resulting in increased ED utilization.29
The results of our study make a unique contribution to the literature on social determinants of health and T2DM outcomes. First, this study examined the association between social needs and DM-specific outcomes on a population level among Medicare patients seeking wellness visits in a large, integrated health care system. Second, this study examined a comprehensive set of social needs, and followed outcomes prospectively in the year after social needs assessment.
While we cannot determine if the relationship between social needs and study outcomes is causal due to the observational study design used in the analysis, our results have implications for clinical care and health care delivery. Based on our findings, further multi-level, multi-sector nterventions are needed to potentially improve outcomes for populations with T2DM and social needs. These interventions should be built on the CMS Accountable Health Communities (AHC) Model implemented in 2016.30 Core components of the AHC model include social needs screening, patient navigation and connection to community-based services, and engagement with community stakeholders to ensure sufficient services are available to address unmet social needs. Further research is warranted on how such interventions impact health outcomes for older adults with T2DM.
The current study has several limitations. First, study results may not be generalizable to settings with different Medicare insurance models, such as noncapitated health care environments (eg, fee-for-service). Second, data on social needs were collected via self-report and may have social desirability biases. Third, the dichotomization of social needs measures limit the ability to asses potential “dose effects” of social needs on study outcomes. Fourth, the population studied was mostly white and non-Hispanic, and was not representative of the US population as a whole. Fifth, results may not be generalizable to noninsured patients or those residing in neighborhoods that have high levels of neighborhood deprivation. In addition, although the relationship between social needs and study outcomes likely did not change during the COVID-19 pandemic period, there may have been more older adults with social needs during this period compared with before the COVID-19 pandemic period. Last, while the population studied is representative of the KPNW Medicare population seeking wellness visits, it may not be generalizable to the KPNW Medicare population overall.
Conclusions and Learnings for Clinical Practice
Our study found that social needs were associated with worse DM-specific outcomes. These results have clear implications for clinical practice. Our study findings suggest the importance of developing further multi-level, multi-sector interventions to address social needs for patients with T2DM. Further research is warranted on how such interventions impact health outcomes for older adults with T2DM.
Acknowledgments
We acknowledge Jill Pope and Neon Brooks for providing editing services to the project and Robin Daily and Mary Early for providing administrative support for the submission of this manuscript.
Notes
This article was externally peer reviewed.
Funding: This work was supported by the National Institutes of Health (NIH) National Cancer Institute (NCI) Grant No. R01CA253028, (C. Kroenke, PI); Kaiser Permanente’s Office of Community Health through the Social Needs Network for Evaluation and Translation (SONNET). SONNET is a national Kaiser Permanente (KP) program that convenes evaluators and researchers from its eight regional care delivery systems; the KP Bernard J. Tyson School of Medicine; KP’s Office of Community Health; the Social Interventions Research and Evaluation Network (SIREN), a KP- and Robert Wood Johnson Foundation–supported network housed at the University of California, San Francisco. SONNET seeks to improve the health of KP members and the communities they live in by developing and implementing new, scientifically driven strategies to shape social health practice and policy; the Northwell, New Hyde Park, NY, Institute of Health System Science, Feinstein Institutes of Medical Research, Manhasset, NY, and Department of Medicine, Manhasset, NY.
Conflict of interest: The authors have no conflicts of interest to report.
To see this article online, please go to: http://jabfm.org/content/38/1/125.full.
- Received for publication April 3, 2024.
- Revision received April 10, 2024.
- Accepted for publication September 16, 2024.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.